

Unsupported: No scientific evidence suggests that the spike protein generated by vaccination causes any harm. Large clinical trials found no evidence that hydroxychloroquine and ivermectin are effective at preventing or treating COVID-19.
Misleading: Contrary to Malone’s claims, COVID-19 vaccines have a high safety profile, and remain effective against severe illness caused by the Omicron variant; a booster dose enhances and prolongs protection.

BEHAUPTUNG: COVID-19 vaccines are “experimental”; hydroxychloroquine and ivermectin are effective COVID-19 treatments; “natural immunity is superior to the vaccine induced immunity”; the vaccine-induced spike protein is dangerous, causes myocarditis, ADE, and infertility; previously-infected people are at “much higher risk” for adverse events after vaccination; COVID-19 vaccines are ineffective, booster doses induce tolerance; “Omicron is a mild variant. It is absolutely able to escape prior vaccination”.
REVIEW
On 31 December 2021, the actor and comedian Joe Rogan interviewed (see full transcript of the interview here) the scientist Robert Malone for The Joe Rogan Experience, a Spotify-exclusive podcast. With an estimated audience of millions of people, Rogan’s podcast is among the most popular worldwide, and the interview went immediately viral on social media.
The link to the interview on Spotify received more than 51,000 interactions on Facebook, Instagram, and Reddit, according to the social media analytics tool CrowdTangle. Full videos and video excerpts also appeared on other platforms like YouTube, which later removed a video of the full interview from the platform.
During the interview, which lasted about three hours, Malone made multiple inaccurate, misleading and/or unsubstantiated claims about COVID-19 treatments and vaccines’ safety and immunity. Malone has repeatedly spread misinformation about COVID-19 vaccines, as multiple reviews by Health Feedback and others (see examples here, here, and here) show. Malone’s account was permanently suspended by Twitter on 29 December 2021, for violating the platform’s policies about COVID-19 misinformation.
Malone’s claims during Rogan’s interview prompted a group of 270 scientists, medical professionals, professors, and science communicators to co-sign an open letter calling on Spotify to „mitigate the spread of misinformation on its platform“. The letter, first reported by Rolling Stone, criticized Malone for promoting conspiracy theories and „falsehoods about COVID-19 vaccines“. It also denounced the podcast’s „concerning history of broadcasting misinformation, particularly regarding the COVID-19 pandemic [see here, and here]“.
This review will address some of the most relevant scientific claims made by Malone during the interview.
Claim 1 (Inaccurate):
“These mandates of an experimental vaccine are explicitly illegal. They are explicitly inconsistent with the Nuremberg Code. They’re explicitly inconsistent with the Belmont Report.”
None of the COVID-19 vaccines currently in use in the U.S. are experimental. Labeling them as so misrepresents their status after being proven safe and effective, as Health Feedback explained before.
The Nuremberg Code was created in 1947 during a trial of Nazi doctors that conducted experiments on concentration camp prisoners. The Belmont Report was published as a result of the U.S. National Research Act of 1974 and outlines the basic ethical principles and guidelines for conducting research on human subjects. Both of them specifically address experimentation on human subjects.
COVID-19 vaccines demonstrated their efficacy and safety in clinical trials before receiving Emergency Use Authorization by the U.S. Food and Drug Administration (FDA). Therefore, as covered in this earlier review, they aren’t experimental, and neither the Nuremberg Code nor the Belmont Report apply to them.
Claim 2 (Unsupported):
“So it’s not just Ivermectin, it’s hydroxychloroquine. […] there’s good modeling studies that [show that] probably half a million excess deaths have happened in the United States through the intentional blockade of early treatment by the US government”
Malone claimed that countries like China, Japan, and India, used hydroxychloroquine and ivermectin effectively to treat COVID-19 patients. He cited the specific case of the Indian state of Uttar Pradesh. After a large second COVID-19 wave in India in April 2021, the state experienced a sharp decline in the number of COVID-19 cases, which some attributed to the government’s recommendation to use ivermectin to treat mild COVID-19 patients. Malone suggested that Uttar Pradesh „crushed COVID“ by deploying early ivermectin treatment among the population.
Health Feedback addressed this claim in this review and found it to be unsupported by scientific data. Large-scale, randomized controlled clinical trials—which are considered the gold standard for evaluating the safety and efficacy of a new intervention—showed no benefit of either hydroxychloroquine[1-4] or ivermectin[5-8] for preventing or treating COVID-19 (see previous reviews here, here, here, and here). Given this lack of evidence, there is no scientific reason to assume that it was ivermectin use and not other factors that caused the drop in COVID-19 cases in Uttar Pradesh. In this article for The Conversation, epidemiologist Rajib Dasgupta hypothesized that this sharp decline could have resulted from a preexisting immunity due to a high rate of infections, combined with a higher COVID-19 vaccination rate.
Malone further claimed that hydroxychloroquine and ivermectin „are among the safest medicines we know“. In support of his claim, he argued that the World Health Organization (WHO) included both of them in the Model List of Essential Medicines. However, this status only applies to the drugs when used at specific concentrations and for specific conditions (see recommended uses for hydroxychloroquine and ivermectin), not as antivirals in COVID-19 patients, as Health Feedback explained in this earlier review. Currently, public health authorities like the WHO and regulatory bodies like the U.S. FDA don’t recommend the use of ivermectin and hydroxychloroquine in COVID-19 patients except in the context of clinical trials.
Claim 3 (Misleading):
“[There are] over 140 studies that document that natural immunity is superior to the vaccine induced immunity”
Malone claimed more than a hundred studies show that infection-induced immunity—which he referred to as natural immunity— is superior to vaccine-induced immunity. As evidence, he cited a study from Israel reporting 13 times fewer infections and fewer hospitalizations in previously infected people compared to fully vaccinated individuals[9].
This earlier review by Health Feedback explained that the study, which is actually a preprint—a manuscript submitted for publication that hasn’t been peer-reviewed by other scientists yet—was affected by several biases that compromised the reliability of the results. For example, high-risk individuals were over-represented in the vaccinated group (selection bias). Also, the authors excluded from the study unvaccinated people who died of COVID-19 (survivorship bias).
There is no doubt that both vaccination and infection can confer protection against future infection, hospitalization, and death. The main difference between the two is that vaccination is safer because it induces immunity without exposing the person to the disease and its associated risks. But arguing that one type of immunity gives better protection than the other, as Malone did, is misleading. As Health Feedback discussed in this Insight article, this debate creates a false dilemma by incorrectly presenting infection and vaccination as mutually exclusive options when they aren’t.
Immunologic data show that the level of protection from prior infection varies greatly from person to person[10,11], and some individuals who recover from infection don’t even develop antibodies. These individuals might remain susceptible to reinfection in the short term. Several studies show that vaccination enhances previous immunity, adding an extra layer of protection against the disease[12,13], just like cars contain multiple safety features, like an airbag, brakes, and seat belts. For this reason, public health authorities like the U.S. Centers for Disease Control and Prevention (CDC) recommend that previously infected people also get vaccinated.
Claim 4 (Misleading):
“[I]t’s very clear that people that have natural immunity have a much higher risk factor for this whole spectrum of adverse events, if they get jabbed”
During the interview, Malone mentioned a number of adverse events, including irregularities of heartbeat, hypertension, narcolepsy, restless leg syndrome, and myocarditis (heart inflammation). He claimed that these events are known and relatively frequent side effects of the COVID-19 vaccines and that previously infected people are at „a much higher risk“ of experiencing them following vaccination than people who weren’t previously infected.
Malone backed up his claims by citing the U.S. Vaccine Adverse Reporting System (VAERS), even though its website explicitly warns against using VAERS reports alone “to determine if a vaccine caused or contributed to an adverse event or illness”.
Data from the U.K. ZOE COVID Symptom Study and a few smaller studies indicate that people who were previously infected are indeed about twice more likely to experience side effects[14,15]. But contrary to what Malone suggested, such effects were generally mild, including fatigue, headache, chills, muscle and joint pain, and fever. None of the studies reported serious side effects requiring hospitalization among previously infected individuals.
Certain side effects are normal after vaccination, and simply indicate that the vaccine is building immunity against the virus. Tim Spector, professor of genetic epidemiology at King’s College London and lead scientist on the ZOE COVID Symptom Study app, commented on the results:
“[S]o far the post vaccine effects we see are mild and in the minority of people. It’s interesting to see that those with previous COVID are more likely to experience these mild after effects than naive subjects. This could be good news, as a larger response like this suggests that those getting a first dose after having had COVID are generating a stronger immune reaction and may get greater protection from just a single shot of the vaccine.”
A study published in the New England Journal of Medicine supports Spector’s comments, showing that a single dose of an mRNA COVID-19 vaccine in previously infected individuals produced antibody levels that were similar, or even higher, than those observed in fully vaccinated people who didn’t have a previous infection[15].
Claim 5 (Misleading):
“The myocarditis was so bad that you went to the hospital. Incidence rate is 1 in 2,700”
Public health authorities, including the U.S. CDC and the WHO, acknowledge myocarditis as a rare side effect of mRNA COVID-19 vaccines, particularly in young male individuals. Malone implied that such cases are quite frequent (up to one case per 2,700 vaccinated individuals) by citing a study conducted in Hong Kong and published in Clinical Infectious Diseases[16].
The cited study evaluated the risk of heart inflammation in adolescents aged 12 to 17 who received a Pfizer-BioNTech COVID-19 vaccine. The incidence cited by Malone applies exclusively to male adolescents who received their second vaccine dose, while the reported overall incidence was one case per 5,400 (18.5 cases per 100,000) vaccinated individuals. As Health Feedback explained in this previous review, this study has an important limitation, in that it relies on data from pharmacovigilance systems, which cannot on their own establish causal associations between the event (heart inflammation) and vaccination.
In addition, the results from this study contrast with the official report on vaccine safety monitoring from the Hong Kong Health Department, which reports 1.6 cases of myocarditis per 100,000 vaccine doses administered. Other studies conducted in the U.S., Israel, and Denmark also show that cases of heart inflammation following COVID-19 vaccination are overall infrequent, ranging from 0.5 to 5.7 cases per 100,000 vaccinated individuals[17-21].
These studies also show that most cases of myocarditis following COVID-19 vaccination are mild and fully recovered within days, contrary to what Malone suggested[22]. In fact, estimates indicate that the risk of myocarditis and cardiac complications is about five times higher after COVID-19 than after vaccination[23].
For all these reasons, the U.S. Advisory Committee on Immunization Practices concluded that “the benefits of COVID-19 vaccination to individual persons and at the population level clearly outweighed the risks of myocarditis after vaccination”. Public health authorities, including the CDC, recommend that “everyone ages five years and older get a COVID-19 vaccine”.
Claim 6 (Incorrect):
“Think twice about giving these jabs to your kids, among other things. Your girls are born with all the eggs they will ever have. And these lipids are going to the ovaries, and they appear to be affecting menstruation in some way.”
Malone implied that mRNA COVID-19 vaccines might impair fertility. Specifically, he claimed that the lipid nanoparticles—the fat droplets containing the mRNA—go to the ovaries „at a very high rate“, up to 11%. As Health Feedback explained in this earlier review, this is inaccurate.
The claim arises from the misinterpretation of data from an official document submitted by Pfizer to Japan’s regulator Pharmaceuticals and Medical Devices Agency (PMDA). The document showed the biodistribution of lipid nanoparticles throughout different tissues in rats that had been previously injected with these particles. Contrary to Malone’s claim, the data clearly showed that the largest concentration of lipid nanoparticles remained at the injection site. In contrast, the peak concentration in the ovaries was only 0.095% of the administered dose.
Some women did indeed report changes in menstrual cycles after COVID-19 vaccination, including longer, heavier, or more painful bleeding. Because vaccine safety trials generally don’t evaluate menstrual irregularities, data about the potential effect of the COVID-19 vaccines in menstruation was lacking.
In January 2022, the first study addressing this issue was published in Obstetrics & Gynecology[24]. The study, involving almost 4,000 women registered in a fertility tracking app, compared menstrual cycle data before and after vaccination. The authors observed an increase in cycle length of less than one day after vaccination compared to pre-vaccination cycles. However, they concluded that this small change is within the range of normal variability, and therefore, the change wasn’t clinically meaningful.
Therefore, Malone’s claim that COVID-19 vaccines impair fertility or ovaries’ normal function is based on misinterpreted data and unsupported assumptions. In contrast, safety data from vaccine monitoring and scientific studies don’t suggest any negative effect of COVID-19 vaccines on fertility, either in men or women[25,26].
Claim 7 (Incorrect):
“The safety signal is there. It is associated with vectors that express spike, whether it’s the vaccine, the virus or the adenovirus, you know, the mRNA, the virus itself or the adenoviral vector spike, those toxicities are there. And the common variable is the spike protein”
Malone suggested that the spike protein, including that generated by mRNA COVID-19 vaccines, is toxic and leads to various adverse effects, from blood clots to brain inflammation and autoimmunity. This claim is incorrect because it is, at least partially, based on 1) the unsupported assumption that high concentrations of the spike protein from vaccination enter the bloodstream, and 2) the results from animal studies reporting the potential toxicity of the spike protein from the virus, not from the vaccine[27-29].
Biophysicist Uri Manor, an assistant research professor at the Salk Institute and co-author of one of these animal studies that Malone cited, explained on Twitter that the amount of spike protein from vaccines in the blood is extremely low compared to the levels found to cause harm in animal studies[30].
Overall, there is no evidence suggesting that the spike protein produced after mRNA vaccination is dangerous in any way, as Health Feedback explained in earlier reviews (see here, here, here, and here).
Claim 8 (Misleading):
“[T]here is signs in some data […] from Denmark, among other places of negative efficacy against Omicron as a function of the number of vaccinations up to three”
The claim that the COVID-19 vaccines have negative vaccine effectiveness (VE), that is, they make people more prone to illness, was covered in this earlier review by Health Feedback. The claim is based on this preprint from a research team in Denmark[31]. The authors used Danish nationwide registries to evaluate the vaccine effectiveness (VE) of the COVID-19 mRNA vaccines against Omicron over time.
The first author of the preprint, medical statistician and epidemiologist Christian Holm Hansen, explained to Health Feedback that the claim misrepresented their results. He said that this effect often arises due to biases, which “are quite common in VE estimation from observational studies based on population data.” These biases include potential differences in detection, testing, or behavior between vaccinated and unvaccinated individuals.
At some point during the interview, Malone acknowledged such biases and further clarified that he was “not saying that this shows that we’re having vaccine-enhanced infection”. Still, he implied a link between negative VE and a phenomenon called antibody-dependent enhancement (ADE). ADE occurs when antibodies against a virus improve the virus’ ability to cause infection, making people more prone to severe illness.
Contrary to the impression given by Malone, COVID-19 vaccines haven’t shown any sign of ADE, as Health Feedback already explained here, here, and here. In fact, all evidence shows precisely the opposite: that COVID-19 vaccines provide a high level of protection against severe illness and death and also reduce the risk of infection, even in the face of the Omicron variant[32-35]. While this variant does reduce VE, particularly against infection, it remains up to 70% effective against hospitalization[35]. A booster dose helps strengthen the immune response.
Claim 9 (Misleading):
“One of those shots, they’re high doses of antigen that are administered repeatedly to your child. And what it does is, induces something that […] we call high zone tolerance.”
High zone tolerance is a phenomenon where the immune system stops responding to an antigen, which is any substance that induces an immune response, after repeated exposure to large amounts of that antigen. Marco Cavalieri, the European Medicines Agency’s head of Biological Health Threats and Vaccines Strategy, explained in a 11 January 2022 press briefing that this phenomenon could be a concern “[i]f we have a strategy in which we give boosters, let’s say, every four months approximately”.
But so far, no evidence indicates that standard administration of COVID-19 vaccines, including boosters, leads to tolerance. On the contrary, Cavalieri said:
“The data on the impact in real life shows that giving a booster dose strengthened the immune response even beyond what was seen with the initial course and restores or extends protection.”
The EMA’s remarks also don’t imply that we should stop boosting. Rather, Cavalieri advocated for extending the time between boosters:
“It would be much better to start thinking about an administration of boosters that are more spaced in time. Ideally, if you want to move towards a scenario of endemicity, then such boosters should be synchronized with the arrival of cold season in each of the hemispheres, similarly to what we are doing with the influenza vaccine.”
Claim 10 (Inaccurate and Misleading):
“Those surrounding States in the Palestinian territory does not (sic) have that level of vaccine uptake at all. The mortality in the surrounding States and the Palestinian Authority is substantially less from this virus than the mortality in Israel”
With this statement, Malone implied that COVID-19 vaccines are ineffective at preventing COVID-19 deaths in Israel, which has a vaccination rate of 65%, compared with the 29.3% of the population fully vaccinated in Palestine (Figure 1). However, the data shows exactly the opposite of what Malone claimed.
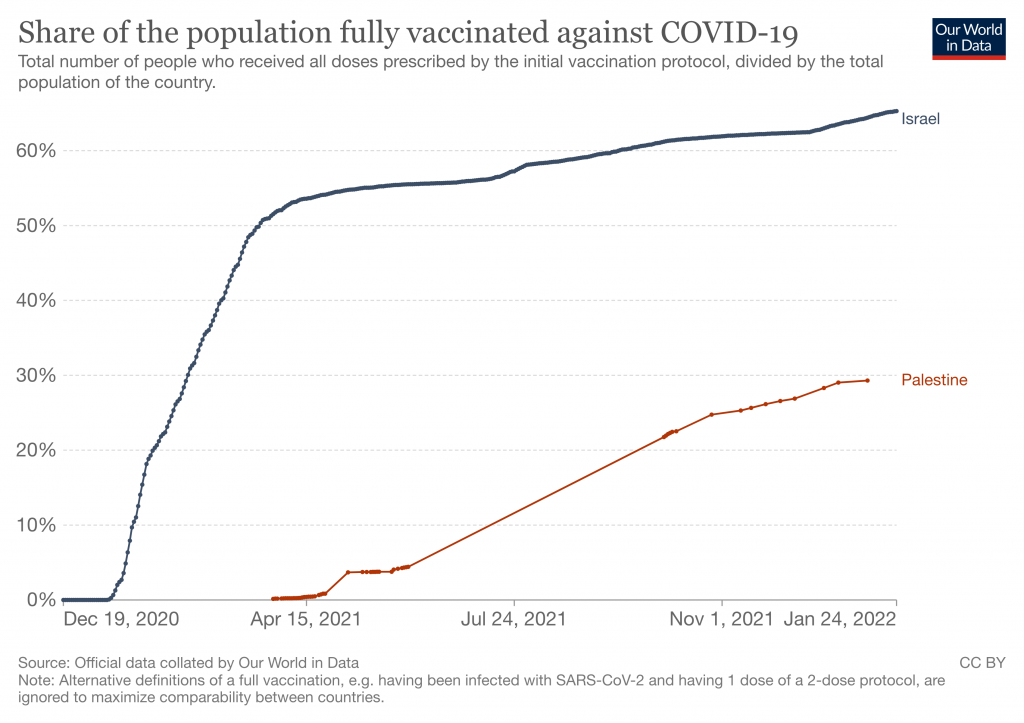
Figure 1. Proportion of fully vaccinated people in Israel and Palestine. Data retrieved on 24 January 2022. Source: Our World in Data.
Firstly, the claim that Palestine has a lower COVID-19 mortality than Israel is inaccurate. At the time Malone made this claim, the cumulative number of confirmed deaths per million population was already higher in Palestine than in Israel, as Figure 2 shows.
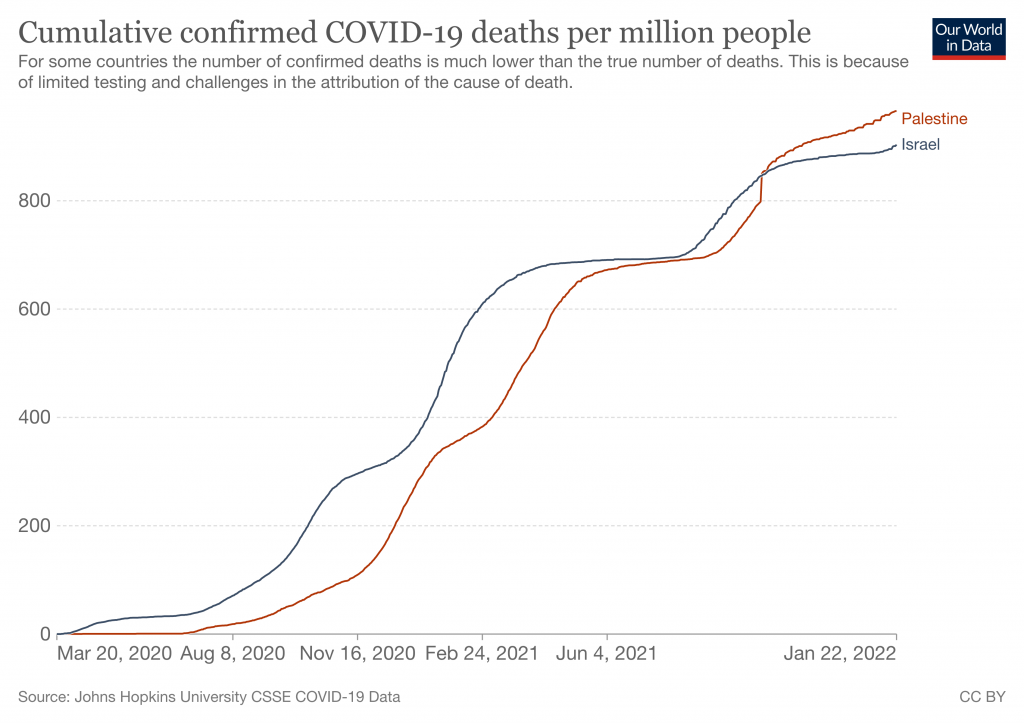
Figure 2. Cumulative confirmed COVID-19 deaths per million people in Israel and Palestine. Data retrieved on 22 January 2022. Source: Our World in Data.
Secondly, simply correlating vaccine coverage with mortality in two countries doesn’t tell us whether a vaccine is effective. Comparing mortality data in different populations can be challenging. Many factors can influence these data, including the demographics and the testing and reporting capacity.
Claim 11 (Missing context):
“[I]t is absolutely looking like Omicron is a mild variant. It is absolutely able to escape prior vaccination […] we are all going to get infected. Whether you use masks or not, use social distancing or not.”
Preliminary data suggest that Omicron is indeed more contagious but less virulent than previous variants. However, some people infected with Omicron still get hospitalized or die. The WHO warns that Omicron should not be dismissed as mild, because a rise in infections worldwide could once again overwhelm health systems. For this reason, it calls for countries to “prevent the spread of Omicron with the proven health and social measures”.
While Omicron reduces COVID-19 vaccine protection against infection and disease, it doesn’t evade immunity completely. Preliminary data from South Africa indicate that two doses of an mRNA vaccine provide up to 70% protection against hospitalization and death[35]. A 31 December 2021 briefing from the U.K. Health Security Agency indicates that, even though vaccine protection against Omicron wanes over time, a booster dose extends this protection and increases vaccine effectiveness against hospitalization to 90%.
Final note
Towards the end of the interview, Malone talked about mass formation psychosis, comparing the situation during the COVID-19 pandemic with the situation in Germany during the 20s and 30s. Several news outlets and fact-checking organizations covered his claim before (see articles by Reuters, AP News, PolitiFact). The term psychosis describes a state of mind that involves some loss of contact with reality. Jay Van Bavel, associate professor of psychology and neural science at New York University, told Reuters that the term mass formation psychosis “doesn’t exist as a real academic concept”.
Other psychologists refuted Malone’s claim as well. Steven Jay Lynn, a psychology professor at Binghamton University in New York, told AP News that the argument that a group can “literally become hypnotized and can be led anywhere” is based on a myth about hypnosis.
There is evidence that groups can influence an individual’s behavior. However, Chris Cocking, principal lecturer at the School of Humanities and Applied Social Sciences at the University of Brighton, explained to Reuters that “[t]he idea that crowds fall under a mass psychosis and are no longer responsible for their actions is a total myth that’s not supported by any credible evidence”.
REFERENCES
- 1 – Self et al. (2020) Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients With COVID-19: A Randomized Clinical Trial. JAMA.
- 2 – The RECOVERY Collaborative Group. (2020) Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. New England Journal of Medicine.
- 3 – WHO Solidarity Trial Consortium. (2020) Repurposed Antiviral Drugs for Covid-19 — Interim WHO Solidarity Trial Results. New England Journal of Medicine.
- 4 – Arabi et al. (2021) Lopinavir-ritonavir and hydroxychloroquine for critically ill patients with COVID-19: REMAP-CAP randomized controlled trial. Intensive Care Medicine.
- 5 – Popp et al. (2021) Ivermectin for preventing and treating COVID‐19. Cochrane Systematic Reviews.
- 6 – Siemieniuk et al. (2020) Drug treatments for covid-19: living systematic review and network meta-analysis. BMJ.
- 7 – Vallejos et al. (2021) Ivermectin to prevent hospitalizations in patients with COVID-19 (IVERCOR-COVID19) a randomized, double-blind, placebo-controlled trial. BCM Infectious Diseases.
- 8 – López-Medina et al. (2021) Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial. JAMA.
- 9 – Gazit et al. (2021) Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections. medRxiv. [Note: This is a preprint that has not yet been peer-reviewed at the time of this review’s publication.]
- 10 – He et al. (2021) Seroprevalence and humoral immune durability of anti-SARS-CoV-2 antibodies in Wuhan, China: a longitudinal, population-level, cross-sectional study. The Lancet.
- 11 – Chia et al. (2021) Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: a longitudinal study. The Lancet Microbe.
- 12 – Wang et al. (2021) Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature.
- 13 – Stamatatos et al. (2021) mRNA vaccination boosts cross-variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science.
- 14 – Raw et al. (2021) Previous COVID-19 infection, but not Long-COVID, is associated with increased adverse events following BNT162b2/Pfizer vaccination. Journal of Infection.
- 15 – Krammer et al. (2021) Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. New England Journal of Medicine.
- 16 – Chua et al. (2021) Epidemiology of Acute Myocarditis/Pericarditis in Hong Kong Adolescents Following Comirnaty Vaccination. Clinical Infectious Diseases.
- 17 – Witberg et al. (2021) Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. New England Journal of Medicine.
- 18 – Mevorach et al. (2021) Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. New England Journal of Medicine.
- 19 – Montgomery et al. (2021) Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiology.
- 20 – Simone et al. (2021) Acute Myocarditis Following COVID-19 mRNA Vaccination in Adults Aged 18 Years or Older. JAMA.
- 21 – Husby et al. (2021) SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study. BMJ.
- 22 – Heymans & Cooper (2021) Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nature Reviews Cardiology.
- 23 – Patone et al. (2021) Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nature Medicine.
- 24 – Edelman et al. (2022) Association Between Menstrual Cycle Length and Coronavirus Disease 2019 (COVID-19) Vaccination: A U.S. Cohort. Obstetrics and Gynecology.
- 25 – Gonzalez et al. (2021) Sperm Parameters Before and After COVID-19 mRNA Vaccination. JAMA.
- 26 – Aharon et al. (2021) mRNA COVID-19 vaccines do not compromise implantation of euploid embryos. Fertility and Sterility.
- 27 – Varga et al. (2020) Endothelial cell infection and endotheliitis in COVID-19. The Lancet.
- 28 – Nuovo et al. (2021) Endothelial cell damage is the central part of COVID-19 and a mouse model induced by injection of the S1 subunit of the spike protein. Annals of Diagnostic Pathology.
- 29 – Lei et al. (2021) SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2. Circulation Research.
- 30 – Ogata et al. (2021) Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clinical Infectious Diseases.
- 31 – Hansen et al. (2021) Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv. [Note: This is a preprint that has not yet been peer-reviewed at the time of this review’s publication.]
- 32 – Scobie et al. (2021) Monitoring Incidence of COVID-19 Cases, Hospitalizations, and Deaths, by Vaccination Status — 13 U.S. Jurisdictions, April 4–July 17, 2021. Mortality and Morbidity Weekly Report.
- 33 – Andrews et al. (2022) Duration of Protection against Mild and Severe Disease by Covid-19 Vaccines. New England Journal of Medicine.
- 34 – Chung et al. (2021) Effectiveness of BNT162b2 and mRNA-1273 covid-19 vaccines against symptomatic SARS-CoV-2 infection and severe covid-19 outcomes in Ontario, Canada: test negative design study. BMJ.
- 35 – Collie et al. (2022) Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. New England Journal of Medicine.
