

AFFIRMATION COMPLETE: “vaccinated children appear to be significantly less healthy than the unvaccinated”
REVIEW
The claim that unvaccinated children are healthier than vaccinated children is common in vaccine-skeptic and anti-vaccine circles. The claim was recently revived on Facebook after a study was published on 22 November 2020 in the International Journal of Environmental Research and Public Health[1]. Articles were also published promoting the study, such as this one by Collective Evolution and this one by Children’s Health Defense, a group that campaigns against vaccination. Both articles went viral on Facebook in early December 2020. These articles have received more than 11,000 interactions on Facebook, according to social media analytics tool CrowdTangle, while the study itself has received another 11,000 interactions.
Several studies were cited to support this claim, two of which were also cited in the latest study published in the International Journal of Environmental Research and Public Health. One of them is a study by Mawson et al. published in 2017, which was replete with methodological errors and flawed statistical analyses, as detailed in this Snopes article. The other was published by journalist Neil Miller and chemical engineer Brian Hooker, which was also found to contain several methodological problems, as covered in an earlier review by Health Feedback.
One of the most significant problems in the study by Hooker and Miller was its failure to account for differences in healthcare-seeking behaviours between vaccinated and unvaccinated children. Vaccination status itself is associated with other factors that can influence health outcomes, but do not result from vaccination itself. For example, vaccinated children are more likely to see a doctor when they feel unwell compared to unvaccinated children for various reasons, such as socioeconomic status, accessibility to healthcare services, and possibly greater trust in healthcare professionals[2,3].
As a result, vaccinated children are much more likely to be diagnosed with medical conditions, even though they are not necessarily more likely to develop such conditions compared to unvaccinated children.
The November 2020 study was published by James Lyons-Weiler, who wrongly claimed that the virus that causes COVID-19 contains a manmade sequence, and Paul Thomas, a pediatrician who has spread vaccine misinformation. Thomas’ medical license was recently suspended by the Oregon Medical Board, on grounds that he breached “the standard of care” and placed “the health and safety of many of his patients at serious risk of harm.”
The study examined the billing and medical records of 3,324 patients from Integrative Pediatrics, a clinic run by Thomas. Of the 3,324 patients, 2,763 received between one and 40 vaccines. To determine if there was a difference in disease burden between unvaccinated and vaccinated children, the authors compared the children based on a new metric created for the study, called Relative Incidence of Office Visits (RIOV).
David Gorski, professor of surgery and Wayne State University and editor of Science-Based Medicine, explained the numerous problems with the authors’ approach in this article, particularly with the use of RIOV, a metric that has not been shown by the authors to be a reliable proxy for disease incidence:
“The authors claim that RIOV ‘reflects the total number of billed office visits per condition per group, reflecting the total disease burden on the group and the population that it represents,’ but no good analysis or references are provided to show that RIOV does, in fact, correlate with disease burden, particularly when using billing data. Doing matched analyses for patients with similar ‘days of care’ (DOC) in the practice, which is claimed to be ‘unbiased’ (excuse me if I doubt this, given that there wasn’t really a good demonstration that […] the choice of children with matched DOC was, in fact, ‘unbiased’) doesn’t change this. If the primary outcome is a new, unvalidated metric, it is incumbent upon the investigator to demonstrate its robustness.”
Gorski also highlighted the possibility that Thomas’ own views on vaccines affect the way that his practice approaches diagnoses of autism:
“Dr. Thomas believes that vaccines cause autism. That right there introduces unconscious bias that could affect how likely he and his staff are to investigate subtle signs of autism and [to refer out] for evaluation based on vaccination status and how likely he is to ascribe various diagnoses to ‘unvaxxed’ children compared to ‘vaxxed’ children. One can easily imagine this bias leading to unvaccinated children to be less likely to be given an autism diagnosis than vaccinated children or to be—dare I say?—brought into the office as often for various conditions that Dr. Thomas attributes to vaccines.”
Ironically, as Gorski pointed out out, the study’s Table 7 (see below) demonstrates that vaccines work, with a statistically significant decrease in the incidence of vaccine-preventable diseases in vaccinated children compared to unvaccinated children.
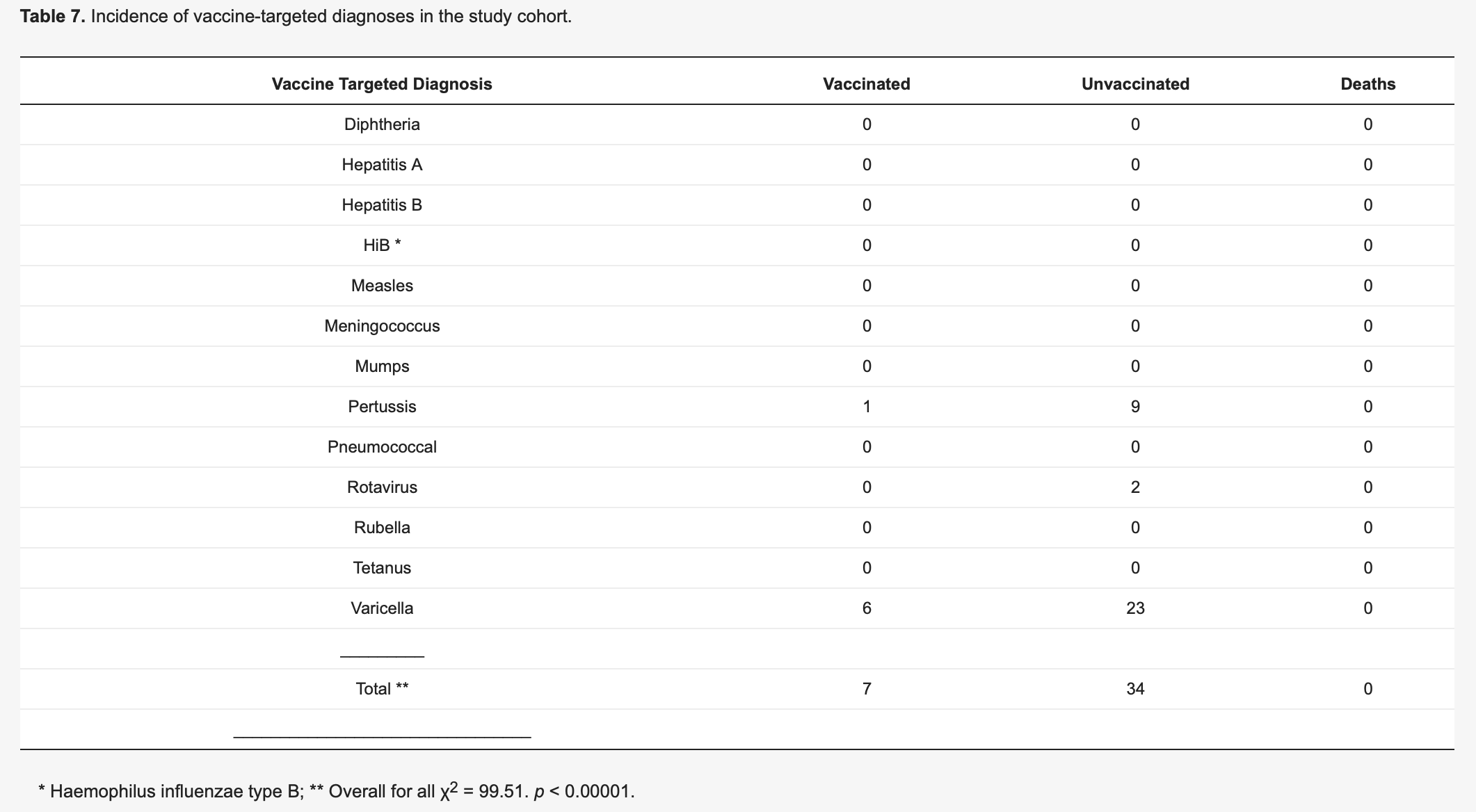
Figure 1. A table from Lyons-Weiler and Thomas’ study. Note that the disease incidence reported in this table is based on the actual number of cases rather than RIOV.
Several well-designed studies examining differences in health and developmental outcomes between vaccinated and unvaccinated children did not detect adverse health outcomes in vaccinated children. A 2004 study in Pediatrics showed no association between vaccines and developmental delay[4]. Another study found that children who were vaccinated in the first year of their lives performed better on cognitive tests[5]. Similarly, children who received measles vaccination in developing countries, specifically Ethiopia, India, and Vietnam, achieved better cognitive test scores than those who didn’t[6]. A 2011 study in Germany, which examined the incidence of allergies and infections among more than 13,000 individuals, did not find adverse health outcomes associated with vaccination[7].
Another study in Germany, published in 2014, examined more than 1,300 individuals and found that vaccination was associated with a significantly lower incidence of asthma[8]. A 2020 Cochrane Review of 138 studies showed no evidence supporting an association of measles, mumps, and rubella vaccination with asthma, bacterial or viral infections, cognitive delay, type 1 diabetes, dermatitis/eczema, and hay fever[9]. At least 20 studies found that vaccines are not associated with autism[4,10-29], as this Health Feedback review discussed.
Vaccines are safe and effective. The U.S. Institute of Medicine concluded in a 2013 review that the childhood immunization schedule is safe[13]. The Vaccine Education Center at the Children’s Hospital of Philadelphia also summarized the scientific evidence showing that vaccines are not associated with a higher risk of asthma or allergies and neurodevelopmental problems like attention deficit/hyperactivity disorder. The American Academy of Pediatricians compiled a list of studies relevant to vaccine safety here.
REFERENCES
- 1 – Lyons-Weiler and Thomas. (2020) Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination. International Journal of Environmental Research and Public Health.
- 2 – Thomson et al. (2016) The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine.
- 3 – Salmon et al. (2005) Factors Associated With Refusal of Childhood Vaccines Among Parents of School-Aged Children: A Case-Control Study. Archives of Pediatrics and Adolescent Medicine.
- 4 – Andrews et al. (2004) Thimerosal Exposure in Infants and Developmental Disorders: A Retrospective Cohort Study in the United Kingdom Does Not Support a Causal Association. Pediatrics.
- 5 – Smith and Woods. (2010) On-time Vaccine Receipt in the First Year Does Not Adversely Affect Neuropsychological Outcomes. Pediatrics.
- 6 – Nandi et al. (2019) Anthropometric, cognitive, and schooling benefits of measles vaccination: Longitudinal cohort analysis in Ethiopia, India, and Vietnam. Vaccine.
- 7 – Schmitz et al. (2011) Vaccination Status and Health in Children and Adolescents: Findings of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Deutsches Ärzteblatt International.
- 8 – Grabenhenrich et al. (2014) Early-life Determinants of Asthma From Birth to Age 20 Years: A German Birth Cohort Study. Journal of Allergy and Clinical Immunology.
- 9 – Di Pietrantonj et al. (2020) Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database of Systematic Reviews.
- 10 – Madsen et al. (2002) A Population-Based Study of Measles, Mumps, and Rubella Vaccination and Autism. New England Journal of Medicine.
- 11 – Institute of Medicine. (2013). Adverse Effects of Vaccines: Evidence and Causality. Retrieved from https://doi.org/10.17226/13164
- 12 – Institute of Medicine. (2013). Childhood Immunization Schedule and Safety: Stakeholder Concerns, Scientific Evidence, and Future Studies. Retrieved from https://doi.org/10.17226/13563
- 13 – Institute of Medicine. (2004). Immunization Safety Review: Vaccines and Autism. Retrieved from https://doi.org/10.17226/10997
- 14 – Fombonne et al. (2006). Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics.
- 15 – Taylor et al. (2014). Vaccines are not associated with autism: an evidence-based meta-analysis of case-control and cohort studies. Vaccine.
- 16 – Ball et al. (2001) An assessment of thimerosal use in childhood vaccines. Pediatrics.
- 17 – Hviid et al. (2003) Association Between Thimerosal-Containing Vaccine and Autism. JAMA.
- 18 – Madsen et al. (2003) Thimerosal and the occurrence of autism: negative ecological evidence from Danish population-based data. Pediatrics.
- 19 – Stehr-Green et al. (2003) Autism and thimerosal-containing vaccines: lack of consistent evidence for an association. American Journal of Preventive Medicine.
- 20 – Verstraeten et al. (2003) Safety of thimerosal-containing vaccines: a two-phased study of computerized health maintenance organization databases. Pediatrics.
- 21 – Thompson et al. (2007) Early Thimerosal Exposure and Neuropsychological Outcomes at 7 to 10 Years. New England Journal of Medicine.
- 22 – McMahon et al. (2008) Inactivated influenza vaccine (IIV) in children <2 years of age: examination of selected adverse events reported to the Vaccine Adverse Event Reporting System (VAERS) after thimerosal-free or thimerosal-containing vaccine. Vaccine.
- 23 – Schechter and Grether. (2008) Continuing increases in autism reported to California’s developmental services system: mercury in retrograde. Archives of General Psychiatry.
- 24 – DeStefano F. (2009) Thimerosal-containing vaccines: evidence versus public apprehension. Expert Opinion on Drug Safety.
- 25 – Tozzi et al. (2009) Neuropsychological performance 10 years after immunization in infancy with thimerosal-containing vaccines. Pediatrics.
- 26 – Price et al. (2010) Prenatal and Infant Exposure to Thimerosal From Vaccines and Immunoglobulins and Risk of Autism. Pediatrics.
- 27 – Barile et al. (2012) Thimerosal exposure in early life and neuropsychological outcomes 7-10 years later. Journal of Pediatric Psychology.
- 28 – DeStefano et al. (2013). Increasing Exposure to Antibody-Stimulating Proteins and Polysaccharides in Vaccines Is Not Associated with Risk of Autism. Journal of Pediatrics.
- 29 – Uno et al. (2012). The combined measles, mumps, and rubella vaccines and the total number of vaccines are not associated with development of autism spectrum disorder: the first case-control study in Asia. Vaccine.
