

Unsupported: No evidence was presented for the assertions that the pandemic was planned or that scientists and/or public health authorities are conspiring to prevent people from getting early treatment. There’s also no evidence for the claim that the spike protein generated by mRNA vaccination is dangerous.

RECLAMACION: the pandemic was planned; the COVID-19 vaccines are experimental; previously infected people have “permanent immunity”; masks don’t work; using three or four doses of vaccine is “wild”; VAERS shows vaccines killed thousands of people, vaccine-induced spike protein causes damage, Omicron comes from vaccinated people
REVIEW
The Joe Rogan Experience, a podcast hosted by actor and comedian Joe Rogan, interviewed cardiologist Peter McCullough in December 2021. During the interview, which spanned about two hours and 45 minutes, McCullough made multiple inaccurate, misleading and/or unsubstantiated claims about the COVID-19 pandemic and the COVID-19 vaccines. This isn’t the first time McCullough propagated health misinformation, as these earlier fact-checks by Health Feedback, Full Fact, and AFP show.
The interview went highly viral on social media. The link to the interview on Spotify received more than 21,000 engagements on Facebook, including more than 9,400 shares. A substantial number of engagements (more than 15,000) also came in from news aggregator and online forum Reddit. This excerpt, posted by the political activist group Young Americans for Liberty, received more than 95,000 views.
This review will cover some of the important claims made by McCullough in the interview.
Claim 1 (Inaccurate):
“The emergency use authorization is a new mechanism or a previously unused mechanism for regulatory pathways of drugs.”
Contrary to McCullough’s claim, the emergency use authorization (EUA) mechanism isn’t new nor was it unused prior to the COVID-19 pandemic. EUAs have been issued by the U.S. Food and Drug Administration (FDA) for tests and medicines long before the pandemic, such as for Ebola and Zika virus, as this FDA page demonstrates.
Claim 2 (Unsupported):
“there was an intentional, very comprehensive suppression of early treatment in order to promote fear, suffering, isolation, hospitalization and death. And it seemed to be completely organized and intentional in order to create acceptance for and then promote mass vaccination.”
“[I]t’s pretty clear that this [pandemic] was planned.”
Throughout the podcast, McCullough claimed the pandemic was planned or that public health authorities and/or scientists conspired for an unnamed reason to keep people from getting treatment. But he never provided any evidence to support these claims. These claims also made regular appearances in Plandemic, a two–part pseudodocumentary that went viral in 2020 and propagated baseless conspiracy theories about COVID-19.
Claim 3 (Inaccurate):
“If you want to see the Johns Hopkins planning seminar called the SPARS Pandemic in 2017, where they had a symposium, people showed up. They wrote up their symposium findings. They published this […] And we’re going to utilize all that in order to railroad the population into mass vaccination. It’s laid out in the Johns Hopkins SPARS pandemic training seminar”
The SPARS Pandemic scenario wasn’t a seminar; rather, it is a “teaching and training resource” published by the Johns Hopkins University Center for Health Security. The document was developed as a self-guided exercise scenario that would enable public health communicators to better manage communication dilemmas regarding medical interventions introduced during a pandemic. The document can be read in full here.
At no point is it stated that the aim of the document is to “railroad the population into mass vaccination” as McCullough claimed. The SPARS Pandemic exercise asks those undertaking the exercise to consider challenges in communication for different kinds of situations that could arise during a pandemic, such as potential vaccine injuries, potential side effects of medical treatments, and the definition of priority groups for vaccines and treatments.
Claim 4 (Lacks context):
“Now they’re saying, no. Now you have to have a third [dose]. And now they’re considering a fourth, which is wild and there’s no end in sight.”
McCullough implied that having to take multiple doses of the COVID-19 vaccine is unusual or unprecedented. This isn’t the case however, as certain childhood vaccines that have been used for decades, like the diphtheria vaccine and the polio vaccine, require four or more doses to complete immunization (see Figure 1).
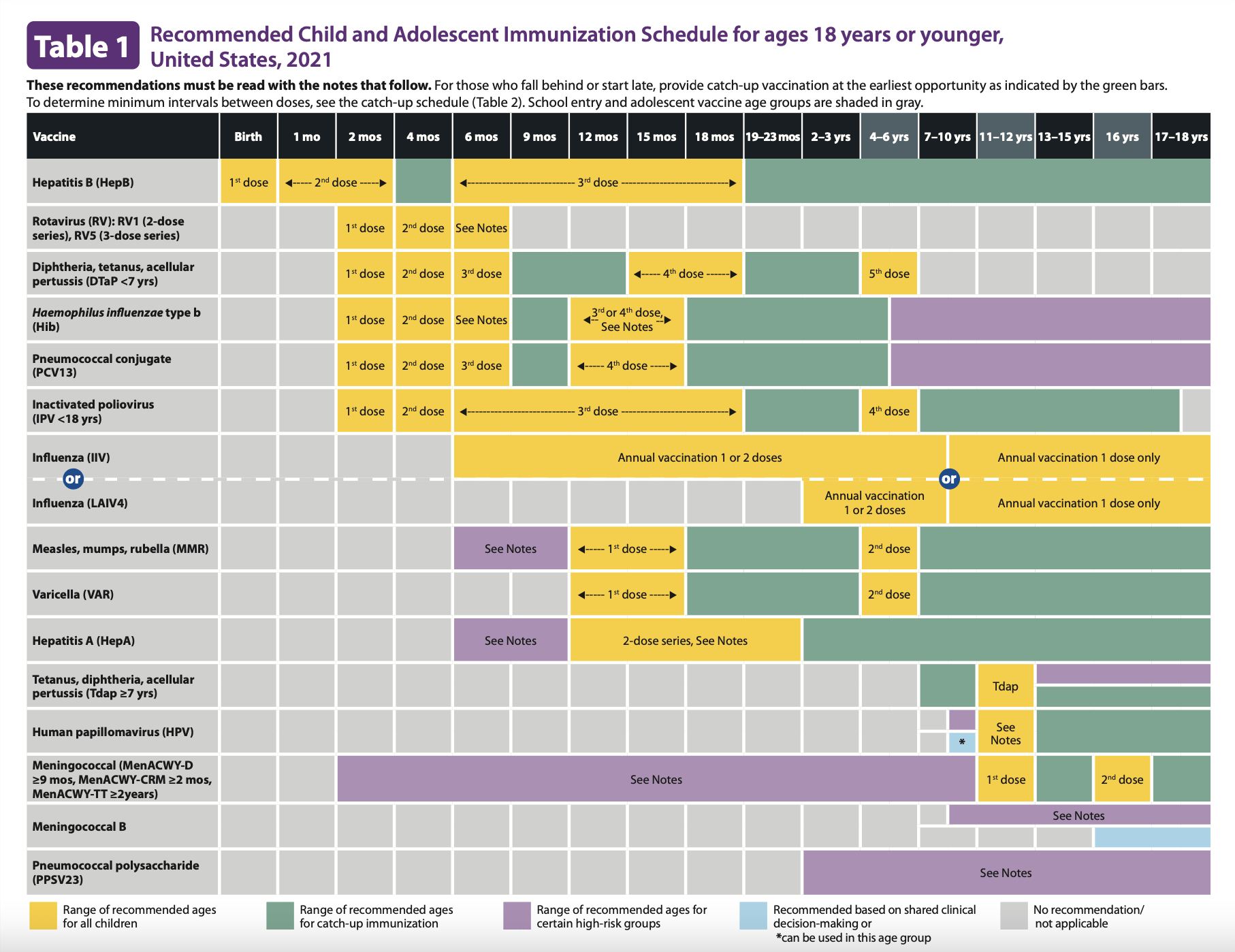
Figure 1. Recommended immunization schedule for children in the U.S., published by the CDC.
Claim 5 (Misleading):
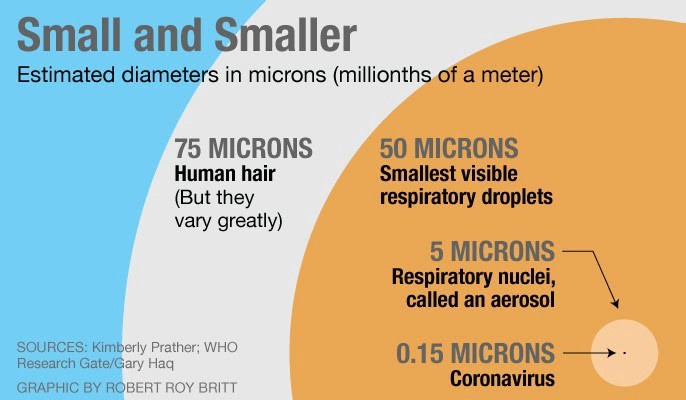
“Masks only filter out about three microns. The virus is one micron.”
The claim that masks don’t work because the pore size is larger than the virus was a popular one in 2020. It was previously reviewed by Health Feedback and found to be misleading. The claim shows a lack of understanding about how virus transmission works. While it is true that a virus particle is smaller than one micron (a millionth of a meter) and thus smaller than the pore size of a mask, virus particles cannot travel in the air on their own. Instead, they need to be carried by liquid droplets, and these are larger than the pore sizes of masks. By blocking the liquid droplets, masks also block the spread of the virus contained within.
Claim 6 (Misleading and Imprecise):
“But one of the original antigenic vaccines that was tested in Australia exposed that HIV epitope. It turned everybody in the trial HIV positive, who took a Covid 19 vaccine in Australia. These young people were outraged. And so this was on the Internet. It was quickly suppressed.”
This is a reference to a COVID-19 vaccine candidate that was being developed by scientists in Australia. Its development was ultimately halted, because certain people who received the vaccine in a safety trial had false-positive results from HIV diagnostic tests. This was because the vaccine candidate used a small portion of a protein from HIV to improve stability of the SARS-CoV-2 spike protein.
It is important to understand that these people weren’t infected with HIV by the vaccine. Instead, they developed antibodies against a particular HIV protein, and these antibodies happened to be the target for certain HIV diagnostic tests. McCullough’s imprecise use of the term “HIV-positive” to describe the vaccine trial participants could give viewers an inaccurate understanding of events, as the term “HIV-positive” is only used to refer to people infected with HIV.
Claim 7 (Inaccurate):
“So one of the big discoveries in 2020 is that the virus is not spread asymptomatically. It’s only spread from sick person to susceptible person. This is a very important two major papers, one by Cao from China, one by Madewell nailed this down.”
McCullough’s claim that “the virus is not spread asymptomatically”, followed by the claim that “it’s only spread from sick person to susceptible person” implies that people who don’t show symptoms cannot spread COVID-19 to others. We know that this isn’t true. Presymptomatic people, who don’t show symptoms initially but develop symptoms later, can transmit the virus even when they aren’t ill. Furthermore, presymptomatic people aren’t the same as asymptomatic people, who never develop symptoms during infection.
It’s unclear exactly which studies McCullough was referring to, but a similar claim that a study by Cao et al. from China[1] showed asymptomatic transmission never occurs had gone viral in 2020 and was addressed in an earlier Health Feedback review. The claim is misleading, as that study assessed the presence of the virus that causes COVID-19 after a stringent lockdown, not the likelihood of asymptomatic transmission.
As with the above study, the reference to Madewell is unclear, but McCullough was perhaps citing this systematic review and meta-analysis by Madewell et al. about household transmission of SARS-CoV-2. However, this study doesn’t support McCullough’s claims either. Madewell et al. concluded that “The lack of substantial transmission from observed asymptomatic index cases is notable”, that is, transmission from asymptomatic people aren’t substantial. But that doesn’t mean that these people don’t transmit as McCullough claimed.
Madewell et al. also added that “presymptomatic transmission does occur, with some studies reporting the timing of peak infectiousness at approximately the period of symptom onset”[2].
Claim 8 (Inaccurate):
“And now our CDC admits finally, through a Free Information Act, lead attorney Aaron Siri pressed the CDC and said, ‘Listen, you’re saying you can get Covid twice. Show us a case, show us a case’. Press, press, press. Finally, the CDC director came out and said, you know what? You can’t get it twice. We’ve never had a single case.”
This is untrue, because reinfections have been documented worldwide, although they are considered uncommon[3-6]. McCullough may have confused this with an earlier claim by lawyer Aaron Siri that previously infected people don’t transmit the virus, based on the CDC’s response to a Freedom of Information request. Siri’s claim was covered by Health Feedback in an earlier review, which found Siri’s claim to be misleading, as he misconstrued a lack of studies determining transmission by previously infected people to be evidence that such people don’t transmit.
Claim 9 (Inaccurate):
“To make matters worse, the CDC has now admitted that the methodology they used for the PCR, originally the CDC methodology that was distributed to all the departments of Community Health and where the laboratory derived assets for the health systems in the early parts of the pandemic cannot distinguish between flu and on Covid 19.”
This is false. The CDC issued a Lab Alert in July 2021, notifying users that the CDC would be withdrawing its request for emergency use authorization for its COVID-19 PCR diagnostic test after December 2021.
This Lab Alert was exploited by certain outlets that misconstrued it as an admission that the PCR test doesn’t work or that it cannot distinguish between COVID-19 and the flu. However, the Lab Alert itself explained that the EUA withdrawal wasn’t due to problems with the performance of PCR tests for detecting COVID-19, but because tests that are capable of processing more samples within a given time and detecting more than one pathogen have since been developed. Such characteristics make these tests the preferred alternatives in the interests of time and resources.
Claim 10 (Inaccurate):
“[O]nce somebody takes a vaccine, the hospitals don’t test them for Covid.”
This isn’t true. The Infection Prevention and Control Recommendations issued by the CDC clearly state that patients are to be tested for COVID-19 regardless of vaccination status if they exhibit symptoms of COVID-19:
“Anyone with even mild symptoms of COVID-19, regardless of vaccination status, should receive a viral test as soon as possible.
Asymptomatic [healthcare personnel] with a higher-risk exposure and patients with close contact with someone with SARS-CoV-2 infection, regardless of vaccination status, should have a series of two viral tests for SARS-CoV-2 infection. In these situations, testing is recommended immediately (but not earlier than 2 days after the exposure) and, if negative, again 5–7 days after the exposure.”
Claim 11 (Inaccurate):
“But in the case where it’s well-documented and you’re sick, you’re done. You basically have permanent immunity.”
It’s false to claim that people who have had COVID-19 develop “permanent immunity”. We know this because reinfections occur[3-6]. Researchers at Imperial College London also obtained data suggesting that the risk of reinfection posed by Omicron is higher than for Delta. This indicates that infection-induced immunity isn’t permanent and the protection it provides will vary depending on the variants in circulation. However, Clive Dix, the former chair of the U.K. Vaccine Taskforce, told Reuters that “we still don’t have sufficient data” and that certain variables, like cellular immune response, weren’t accounted for in the study.
Claim 12 (Inaccurate):
“The vaccines are research. They are all investigational research. And so nobody can encourage somebody to take a vaccine. By the way, that violates the Nuremberg Code.”
At this point in time, the COVID-19 vaccines are no longer investigational. Their safety and efficacy were established in clinical trials involving tens of thousands of people before EUAs were granted[7,8]. Furthermore, the Pfizer-BioNTech COVID-19 vaccine now has full FDA approval.
COVID-19 vaccination campaigns don’t violate the Nuremberg Code either, as Health Feedback explained previously. The Nuremberg Code specifically addresses experimentation on human subjects and was created in 1947 during a trial of Nazi doctors that conducted experiments on concentration camp prisoners. But COVID-19 vaccines aren’t experimental, therefore the Nuremberg Code doesn’t apply.
Attempts to draw parallels between the rigorously tested COVID-19 vaccines and Nazi human experimentation exploit emotional reactions and falsely associate vaccination campaigns using rigorously-tested vaccines with unethical human research in order to promote vaccine hesitancy.
Indeed, the phenomenon of invoking the Holocaust by many of those opposing COVID-19 vaccines and public health measures has grown increasingly popular, as news reports show. A joint statement between UNESCO and the International Holocaust Remembrance Alliance (IHRA) deplored this phenomenon, calling it a form of Holocaust distortion, warning that “Regardless of its form, Holocaust distortion always helps Holocaust denial, antisemitism, conspiracy myths and populism thrive”.
Claim 13 (Inaccurate):
“The CDC and FDA didn’t have any safety review.”
This is false. Simply reading the first page of the FDA Decision Memorandums for the COVID-19 vaccines that are currently in use clearly shows that the clinical trial data was reviewed for safety by medical doctors and scientists (Pfizer-BioNTech, Moderna, and Johnson & Johnson).
Claim 14 (Misleading):
“We’re at 18,000 deaths. And this is just the VAERS, which is underreported.”
This is an example of how the Vaccine Adverse Event Reporting System is commonly misused (VAERS). VAERS makes it very clear that the reports in its database don’t on their own constitute evidence that the vaccine caused the adverse event:
“VAERS is not designed to determine if a vaccine caused a health problem, but is especially useful for detecting unusual or unexpected patterns of adverse event reporting that might indicate a possible safety problem with a vaccine. This way, VAERS can provide CDC and FDA with valuable information that additional work and evaluation is necessary to further assess a possible safety concern.”
Scientists rely on many other indicators aside from temporality to infer causal events, which is extensively covered in an Insight article by Health Feedback.
Claim 15 (Inaccurate):
“We now know that the spike protein after these vaccines is produced in the body for an uncontrolled quantity and an uncontrolled duration of time […] a paper by Ogata and colleagues from Harvard which showed that the free-floating spike protein was in the plasma for an average two weeks after the vaccines […] So that’s spike protein-emia in the plasma. The spike protein damages cells. It damages cells in the heart, the brain, damages blood vessels, causes blood clotting.”
This is a misrepresentation of the findings by Ogata et al[9]. As explained in this Health Feedback review, the study was done in 13 people who had received the Moderna COVID-19 vaccine. Uri Manor, a biophysicist and assistant research professor at the Salk Institute, explained on Twitter that the researchers found that the average amount of spike protein in the blood was about 30 to 40 picograms/mL (one picogram is one trillionth of a gram) and that it disappeared after a few days. No detrimental effects were reported in the study from these levels of spike protein.
Claim 16 (Inaccurate):
“Think about an antiviral monoclonal antibody. What a wonderful advance. We’ve never had it before.”
That’s not true. Monoclonal antibodies developed for antiviral use have been around for several years, as this 2015 review published in the journal Trends in Microbiology shows[10]. One example of an antiviral monoclonal antibody is Palivizumab, which was approved by the FDA in 1998 and is used for preventing respiratory syncytial virus infection in children.
Claim 17 (Unsupported):
“Omicron has actually arisen from the vaccinated, the kids that were passing the Botswana border, they were fully vaccinated.”
The variant was first reported by Botswana in four fully vaccinated people, but the variant could have been circulating for a while before scientists discovered it. Therefore, we don’t know yet whether the Omicron variant originated in a vaccinated person and there’s no evidence supporting this claim to date. Scientists have various hypotheses for how the Omicron variant might have come about, such as chronic infection in an immunocompromised person, a human population that was overlooked during surveillance, or in animals, but nothing is certain yet.
Claim 18 (Accurate):
“The spike protein is so mutated with Omicron, that actually the primer drops out of the PCR patterns, it’s called S gene drop out. So this is the first time based on – depends on what PCR is done – that actually the PCR itself could give a hint that it’s Delta. Otherwise PCRs just tell you, SARS-CoV-2 positive or negative. And then we have to wait for the public health labs to do the sequencing to tell us what variant it is. This case, the PCR test could give us a signature.”
This is true. PCR tests for SARS-CoV-2 detect the presence of the virus by using primers that recognize known genetic sequences of the virus. Certain PCR tests can detect several viral genes. However, in cases where the virus carries multiple mutations in a genetic sequence targeted by the primers, the test can fail to detect the presence of that gene, although other genes are still detectable by the test. The genes detected will depend on the type of test used.
In the case of the Omicron variant, which carries multiple mutations in its spike protein gene (S gene), certain PCR tests can still detect other genes but not the S gene. This phenomenon is termed S gene dropout or S gene target failure. It is a signature that can suggest the variant is Omicron, but it isn’t proof positive that the virus is Omicron, as the Alpha variant also exhibits S gene dropout. However, given that Omicron is more dominant than Alpha, a sample showing S gene dropout is more likely to be Omicron than Alpha. Confirming that a variant is Omicron will still require whole genome sequencing.
READ MORE
Physician Zubin Damania, who also goes by the name ZDoggMD, published a rebuttal of McCullough’s claims on his podcast.
REFERENCES
- 1 – Cao et al. (2020) Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nature Communications.
- 2 – Madewell et al. (2020) Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Network Open.
- 3 – Cavanaugh et al. (2021) Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination – Kentucky, May-June 2021. Mortality and Morbidity Weekly Report.
- 4 – Abu-Raddad et al. (2021) Severity of SARS-CoV-2 Reinfections as Compared with Primary Infections. New England Journal of Medicine.
- 5 – Sheehan et al. (2021) Reinfection Rates Among Patients Who Previously Tested Positive for Coronavirus Disease 2019: A Retrospective Cohort Study. Clinical Infectious Diseases.
- 6 – Vitale et al. (2021) Assessment of SARS-CoV-2 Reinfection 1 Year After Primary Infection in a Population in Lombardy, Italy. JAMA Internal Medicine.
- 7 – Polack et al. (2020) Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. New England Journal of Medicine.
- 8 – Baden et al. (2020) Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. New England Journal of Medicine.
- 9 – Ogata et al. (2021) Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clinical Infectious Diseases.
- 10 – Pelegrin et al. (2005) Antiviral Monoclonal Antibodies: Can They Be More Than Simple Neutralizing Agents? Trends in Microbiology.
