

Cherry-picking: Multiple large-scale studies reported an increased risk of cardiovascular complications associated with COVID-19, including myocarditis and pericarditis, which are ignored by claims like this.

RECLAMACION: ‘Covid “vaccines” cause myocarditis and pericarditis but Covid infections do not. Huge 500k+ participant study. We were lied to, again.’
REVIEW
Social media posts began circulating in September and November 2022, claiming that COVID-19 doesn’t increase the risk of myocarditis and pericarditis, despite evidence showing otherwise. These are conditions in which the heart becomes inflamed.
The study cited to support this claim, titled “The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study”, was published by Tuvali et al. in April 2022 in the Journal of Clinical Medicine[1].
In brief, the authors compared the frequency of myocarditis and pericarditis diagnoses between people who had tested positive for COVID-19 and those who had tested negative. More than 780,000 adults in Israel were included in the study. Diagnoses were identified based on medical records. Notably, only diagnoses made at least ten days after the positive SARS-CoV-2 test were included.
Based on their analysis, the authors reported that “We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection”[1].
This was construed by some social media users to mean that COVID-19 didn’t increase the risk of myocarditis and pericarditis, unlike COVID-19 vaccines—the corollary being that getting COVID-19 is safer than COVID-19 vaccines. Examples of such posts are this tweet by lawyer Marina Medvin and a Facebook post by Australian Senator Malcolm Roberts. Medvin’s tweet in particular was retweeted more than 15,000 times.
However, the study contains important limitations, and such interpretations of the study are inaccurate and misleading, as we will explain below.
The study’s inclusion criteria for myocarditis and pericarditis cases was limited and only involved recovering patients
As stated above, the study only included diagnoses of myocarditis and pericarditis that occurred at least ten days after a person tested positive for SARS-CoV-2 infection. The authors did this because they wished to study “the incidence of myocarditis and pericarditis in a large cohort of COVID-19 patients after recovering from the acute infection” [emphasis added].
Therefore, the study didn’t capture cases of myocarditis and pericarditis if these occurred during the acute phase of the infection, that is, when the patient had COVID-19. Internal medicine physician Jonathan Laxton pointed out this issue in a tweet:
Oh Eli, please stop cherry-picking studies you like. Can you explain to me why they only examined patients 10 days AFTER a positive PCR? Kind of weird when you can get myocarditis during acute COVID, don't you think?
— Jonathan Laxton MD, FRCPC (@dr_jon_l) November 8, 2022
This is an important caveat, because as the authors themselves acknowledged: “It has recently been reported that the incidence of myocarditis and pericarditis is increased in COVID-19 patients during the acute illness” [emphasis added]. This acknowledgement contradicts the claim that COVID-19 doesn’t increase the risk of heart inflammation made in these social media posts.
Another significant caveat about the study is the authors’ choice of diagnostic codes used to identify myocarditis and pericarditis diagnoses in medical records. The authors stated that they used the ICD-10 codes I40, I40.9, I51.4 for myocarditis, and I30, I30.0, and I30.9 for pericarditis. ICD stands for the International Classification of Diseases. According to the World Health Organization:
“Clinical terms coded with ICD are the main basis for health recording and statistics on disease in primary, secondary and tertiary care, as well as on cause of death certificates. These data and statistics support payment systems, service planning, administration of quality and safety, and health services research. Diagnostic guidance linked to categories of ICD also standardizes data collection and enables large scale research.”
However, the authors’ chosen diagnostic codes don’t capture all myocarditis and pericarditis cases. Critically, as Susan Oliver, a scientist who studies materials for medical use, pointed out in a YouTube video, the authors didn’t include diagnostic codes for viral myocarditis (B33.22) and infective myocarditis (I40.0) (see Figure 1 below). Thus, if a patient had tested positive for SARS-CoV-2 and developed myocarditis afterwards, their case might not have been included, since COVID-19-associated myocarditis is the result of an infectious disease caused by a virus.
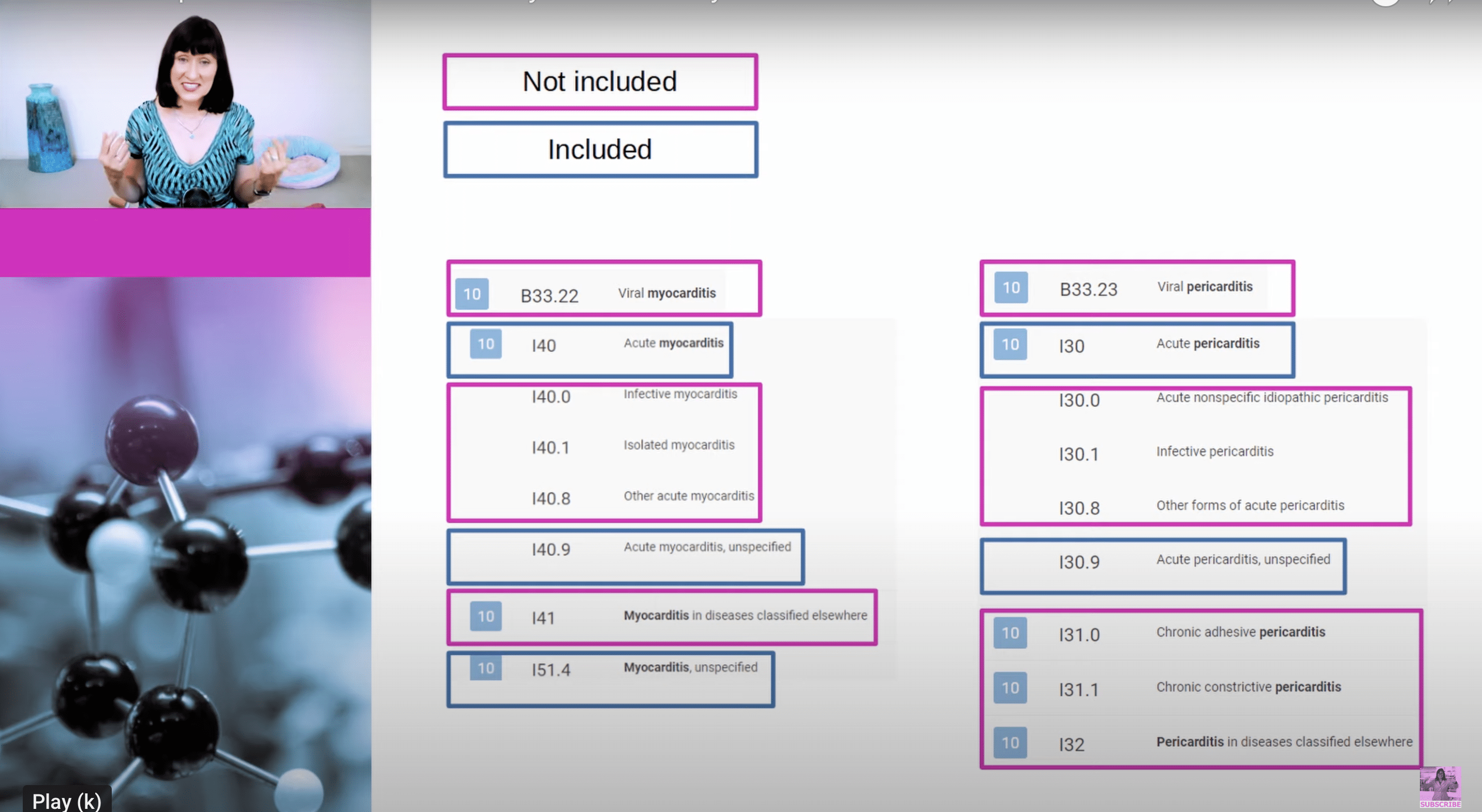
Figure 1. Screenshot of some of the ICD-10 diagnostic codes for myocarditis and pericarditis. Those in blue boxes were included by the study authors, but those in pink boxes weren’t. Source: Susan Oliver.
Oliver also highlighted that the inclusion of only a subset of relevant ICD codes may have led the authors to identify only a small number of cases, which the authors acknowledged as a limitation: “although the potential number of participants who were considered for inclusion was large, the number of cases of myocarditis and pericarditis was small”.
Health Feedback reached out to the authors of the study for comment, and will update this review if new information becomes available.
Apart from the choice of diagnostic codes, the way that the authors defined the control group, specifically as people who tested negative for COVID-19, could also have inadvertently influenced the findings.
“At first glance, this seems like a reasonable criteria, until you consider that a key reason for getting a COVID-19 test is because you have symptoms that resemble COVID-19,” said Oliver.
Even if these people didn’t have COVID-19, they likely had some other infection. And this is relevant since a viral infection is one of the most frequent causes of myocarditis.
In other words, one possible reason the authors didn’t detect an increased risk in COVID-19 patients is that these patients were compared to a control group that was made up of many people who were also at an elevated risk of myocarditis and pericarditis. But it’s also important to consider that people do take COVID-19 tests for other reasons apart from COVID-19-like symptoms, such as to comply with requirements for travel.
In any event, the authors didn’t address this potential issue in their study, casting doubt over the reliability of their findings.
Multiple large-scale studies showed that COVID-19 increases the risk of cardiovascular complications
The attention that this study gained in certain quarters may have to do in part with how it appears—at least on the surface—to provide scientific evidence justifying COVID-19 vaccine skepticism. If it were true that COVID-19 didn’t actually increase the risk of cardiovascular problems, this would overturn in part the basis of COVID-19 vaccine recommendations, which are predicated on the vaccines’ benefits outweighing their risks.
And the fact that COVID-19 vaccines are associated with an increased risk of myocarditis and pericarditis, especially in young men, is well-known and a subject of continued study, as NBC News reported on 12 November 2022.
However, the claim that COVID-19 doesn’t increase the risk of heart inflammation, founded on this study, requires us to discard multiple other published studies that reported the opposite.
For example, a study on the Pfizer-BioNTech COVID-19 vaccine published in the New England Journal of Medicine, also performed in Israel, analyzed data from more than 1.7 million vaccinated people and more than 230,000 people who were infected with SARS-CoV-2[2].
The authors reported that while vaccination increased the risk of myocarditis and pericarditis about three-fold relative to unvaccinated people, SARS-CoV-2 infection increased this risk even more. Infected people had an 11-fold higher risk of myocarditis and pericarditis relative to uninfected people (see Figure 2).
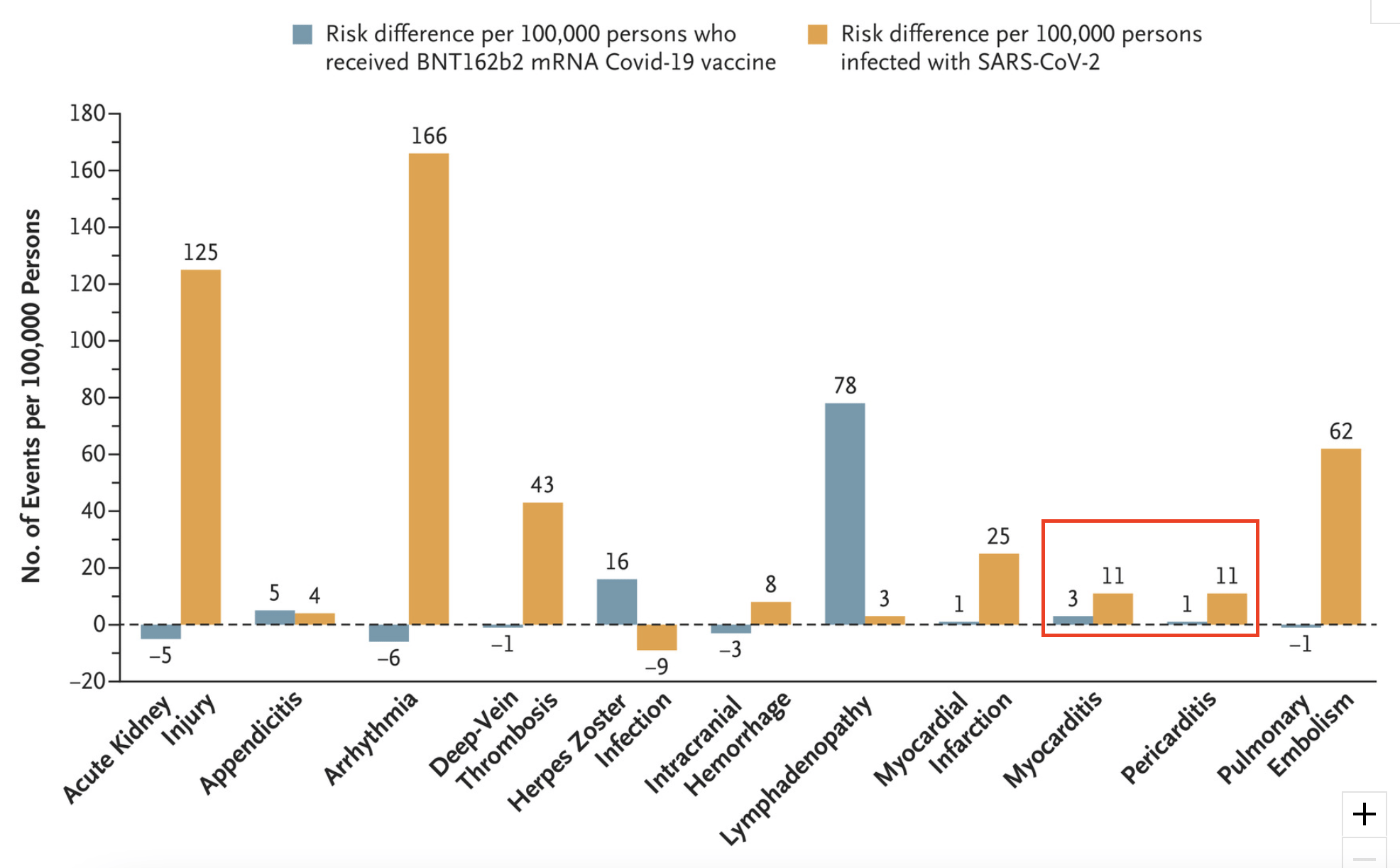
Figure 2. The absolute excess risk of various adverse events after vaccination or SARS-CoV-2 infection[2]. Adapted from the original figure by Barda et al. Note that the effects of vaccination and of SARS-CoV-2 infection were estimated with different cohorts: vaccinated people were compared with unvaccinated people, while those who tested positive for SARS-CoV-2 were compared with uninfected people. Thus, the risks from vaccination and that of infection cannot be directly compared.
Another study, performed in England and which included more than 42 million people, also reported that the risk of myocarditis increased after vaccination, “but was lower than the risks after a positive SARS-CoV-2 test before or after vaccination”[3] (see Figure 3).
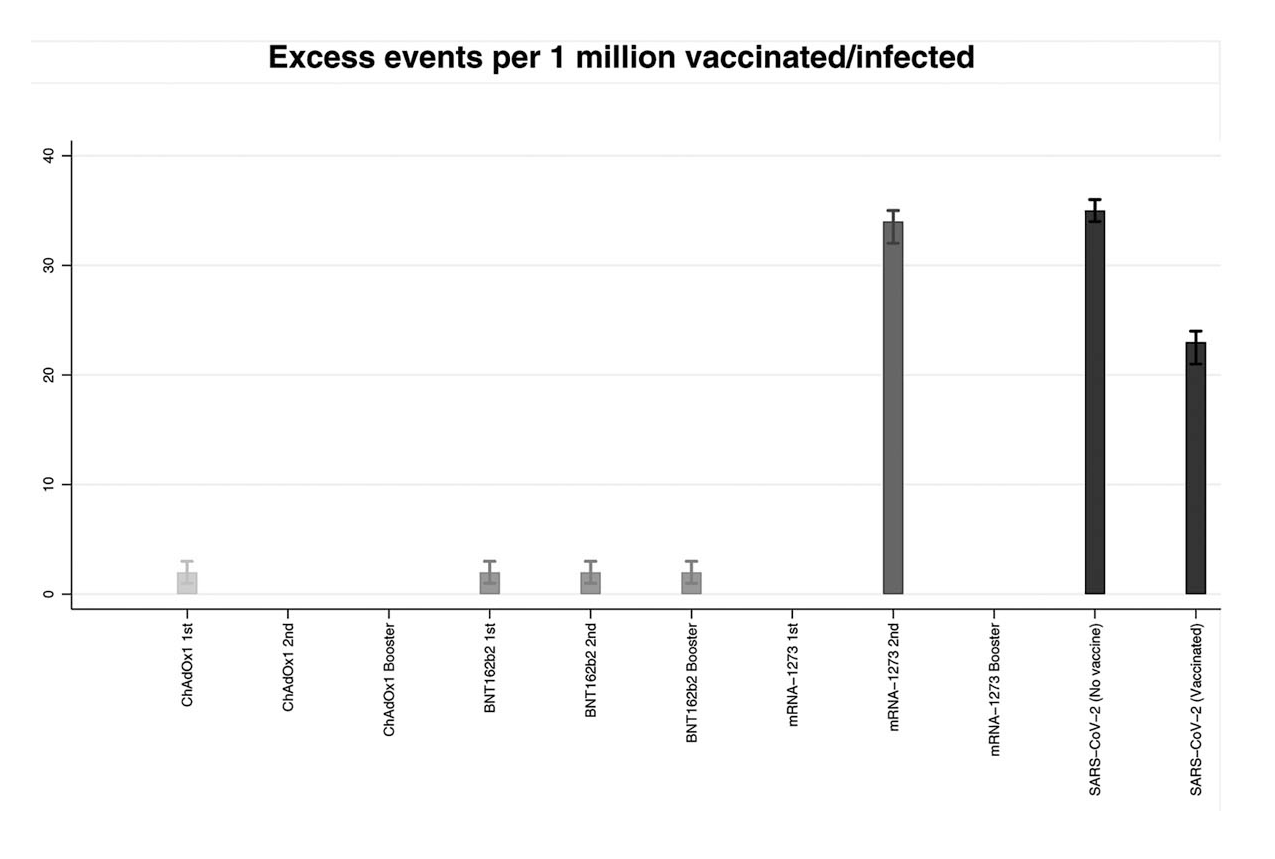
Figure 3. Risk of myocarditis in the 1 to 28 days after COVID-19 vaccines or SARS-CoV-2[3]. Adapted from the original figure by Patone et al. In general, the risk of myocarditis was higher for people who had a SARS-CoV-2 infection compared to the risk following vaccination, except with a second dose of the Moderna COVID-19 vaccine.
A study which analyzed healthcare records of more than 10 million U.S. veterans reported that individuals who had COVID-19 were more prone to developing cardiovascular problems, and that this risk remained even 12 months after infection[4].
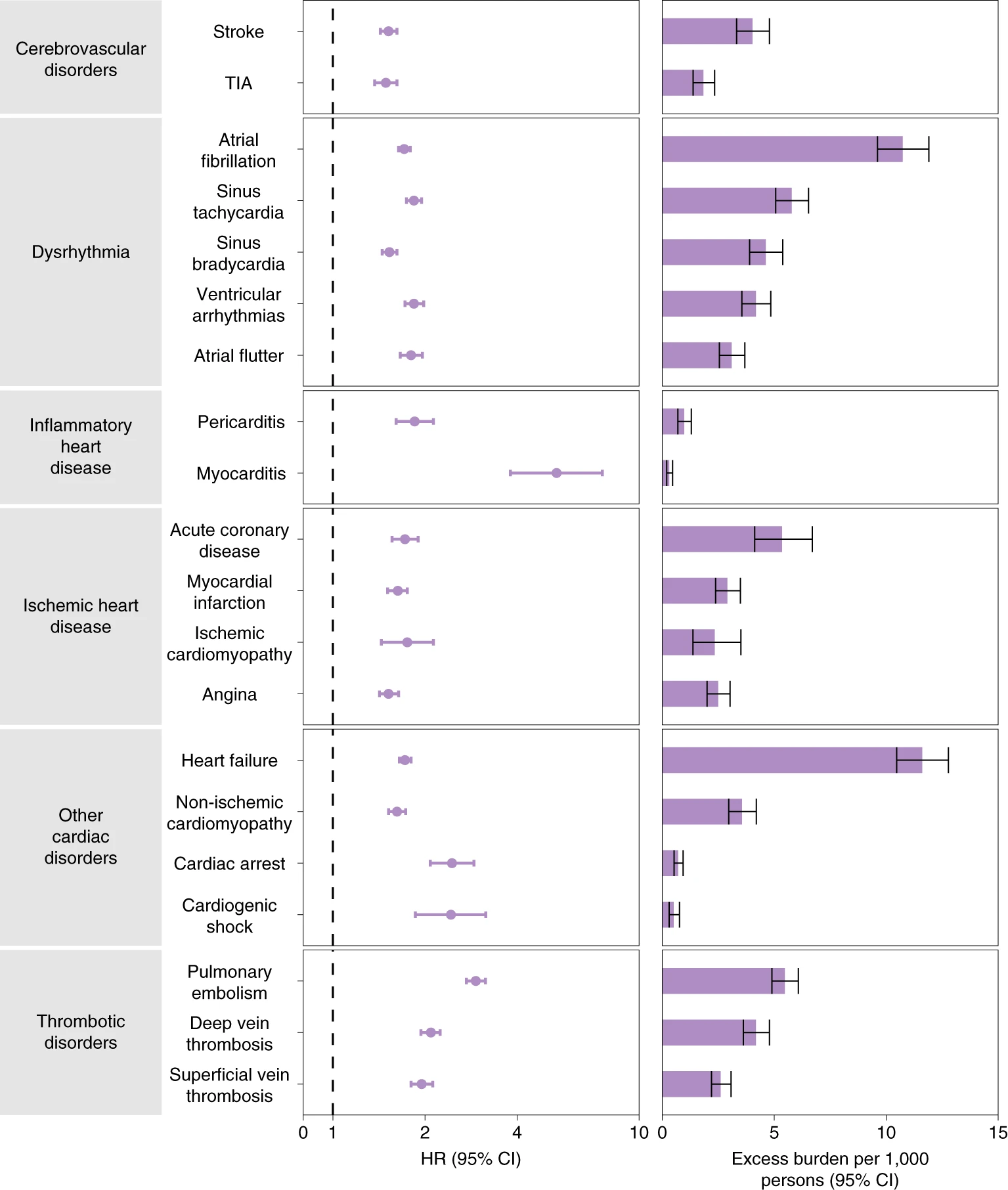
Figure 4. Risks and 12-month burdens of incident post-acute COVID-19 cardiovascular outcomes compared with people who had no evidence of SARS-CoV-2 infection[4]. Outcomes were ascertained 30 days after the COVID-19-positive test until the end of follow-up. Hazard ratios are presented on the left. On the right, the length of the bars represents the excess burden per 1,000 persons at 12 months.
Overall, the study by Tuvali et al. doesn’t provide sufficient evidence for the claim that COVID-19 doesn’t increase the risk of myocarditis and pericarditis, owing to limitations associated with its design. It’s also insufficient to overturn the scientific studies reporting that COVID-19 does increase the risk of myocarditis and pericarditis, and that this risk exceeds that of the risk from COVID-19 vaccination.
REFERENCES
- 1 – Tuvali et al. (2022) The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. Journal of Clinical Medicine.
- 2 – Barda et al. (2021) Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. New England Journal of Medicine.
- 3 – Pantone et al. (2022) Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation.
- 4 – Xie et al. (2022) Long-term cardiovascular outcomes of COVID-19. Nature Medicine.
