
Inadequate support: Rogers’ claim that more children would die from the COVID-19 vaccination than from COVID-19 rests on an incorrectly calculated metric called number needed to vaccinate and a misleading use of vaccine adverse event reports.

RECLAMACION: “For every one child saved by the shot, another 117 would be killed by the shot. The Pfizer mRNA shot fails any honest risk-benefit analysis in children ages 5 to 11.”; Based on VAERS, “there are 128 reports of fatal side effects following coronavirus mRNA injections in people 12 to 24. (That’s through October 22, 2021)”
REVIEW
On 1 November 2021, political economist Toby Rogers published an article on Substack claiming that the Pfizer-BioNTech COVID-19 vaccine would kill more children than it would save. Rogers arrived at this claim based on his calculation of a metric known as “number needed to vaccinate” (NNTV, also abbreviated as NNV) and reports to the U.S. Vaccine Adverse Events System (VAERS). Rogers’ claim was picked up by websites such as Gateway Pundit, which is labeled as a Questionable Source by Media Bias/Fact Check.
Individuals who previously spread vaccine misinformation, like Steve Kirsch and James Lyons-Weiler, also broadcasted the claim to their followers (see here and here). Based on the social media analytics tool CrowdTangle, Rogers’ own article received more than 3,500 engagements on Facebook to date, but his claim reached a wider audience thanks to others who amplified it. For example, Gateway Pundit’s article received more than 5,300 engagements on Facebook.
It’s not the first time that the concept of NNTV and vaccine adverse event reports have been used to promote doubt about COVID-19 vaccine safety. Health Feedback previously fact-checked a similar claim that also went viral and found it to be unsupported. Rogers’ own claim also suffers from the same issues that Health Feedback pointed out in that earlier review, in addition to other problems. Specifically, Rogers incorrectly treated vaccine adverse event reports about deaths as evidence of COVID-19 vaccines causing deaths. As has been explained before and also explicitly stated on the VAERS website: adverse event reports alone don’t constitute evidence that the adverse event was caused by the vaccine.
NNTV originates from an epidemiological metric known as “number to treat”, which is the number of people that need to be treated in order to avoid a specific bad outcome, like death: “if a drug has an NNT of 5, it means you have to treat 5 people with the drug to prevent one additional bad outcome”. Similarly, NNTV is the number of people that need to be vaccinated in order to avoid a bad outcome like death. We can calculate NNTV by dividing 1 with the absolute risk reduction. Another way to arrive at NNTV is to divide 1 with the product of the incidence rate in a given time and vaccine effectiveness, since multiplying the incidence rate with vaccine effectiveness provides the absolute risk reduction[1].
The incidence of COVID-19 deaths among children is a proportion of COVID-19 deaths in children among only infected children. Therefore, if we applied NNTV to Rogers’ target group, we would divide only the number of infected children aged between five and 11 in the U.S. with the product of vaccine effectiveness and number of COVID-19 deaths in this particular population.
But in his calculation of NNTV, Rogers simply divided the number of children aged five to 11 in the U.S. with his calculated figure for the number of lives saved. To quote him:
“[I]njecting all 28,384,878 children ages 5 to 11 with two doses of Pfizer (which is what the Biden administration wants to do) would save, at most, 45 lives (0.8 effectiveness x 57 fatalities that otherwise would have occurred during that time period = 45).
So then the NNTV to prevent a single fatality in this age group is 630,775 (28,384,878 / 45). But it’s a two dose regimen so if one wants to calculate the NNTV per injection the number doubles to 1,261,550. It’s literally the worst NNTV in the history of vaccination.”
Based on his method, it’s clear that Rogers’ NNTV is meaningless because he used the wrong formula. This is made inexplicable by the fact that Rogers is aware of the correct formula to calculate NNTV. We know this, because in the same article, he went on to contend with the NNTV reported in a 2 November 2021 presentation by Sara Oliver, an official with the U.S. Centers for Disease Control and Prevention. Here, he stated that “NNTV is calculated by dividing 1 by the Absolute Risk Reduction”. But when it came to his own calculation of NNTV, he didn’t employ the same method.
Oliver’s presentation reported NNV to prevent one COVID-19 hospitalization as 8,187, based on epidemiology averaged across the whole pandemic. Rogers called the NNV “dishonest and a violation of scientific norms”, because according to him, “There was no Absolute Risk Reduction in hospitalizations in the Pfizer clinical trial in kids 5 to 11, because no one was hospitalized in either the treatment or control group. 1/0 is ‘undefined’ not 8,187.”
Characterizing the CDC’s NNV in this manner is a misrepresentation of events, given that the data used for the NNV calculations presented by Oliver didn’t come from the Pfizer clinical trials and was clearly stated to have originated from the CDC COVID Data Tracker, which records cases, deaths, and hospitalizations in different age groups in the U.S. (see the slide below)—epidemiological data which are used to calculate NNTV, as we explained above. The assumptions for vaccine effectiveness against different outcomes, like hospitalization, were also clearly stated in the presentation.
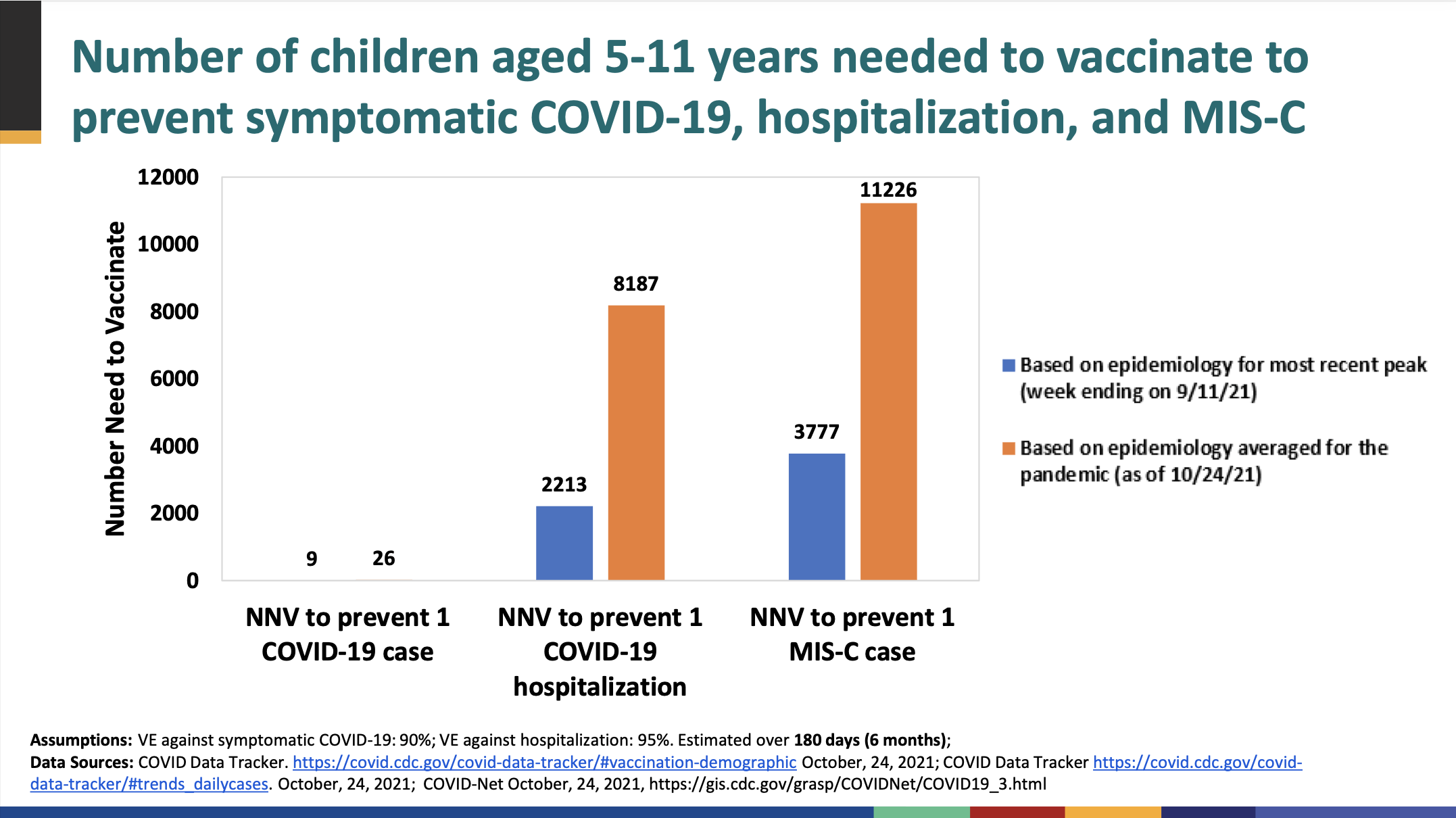
NNTV presented during a 2 November 2021 Advisory Committee on Immunization Practices meeting. The full presentation can be found here.
Overall, Rogers’ claim that he provided “proof” that “more children will die from the vaccine than will die from COVID” is inaccurate. The figures produced by Rogers were calculated wrongly, but exploited by some to lend credibility to false claims about the COVID-19 vaccine safety.
Contrary to Rogers’ claim, scientific evidence from clinical trials demonstrate that the Pfizer-BioNTech COVID-19 vaccine is safe and effective in children. In this article for The Conversation, Debbie-Ann Shirley, an associate professor of pediatrics at the University of Virginia, explained how the COVID-19 vaccines were tested in clinical trials for children. Shirley explained:
“The Pfizer trial for those under age 12 began with three different doses; ultimately, researchers determined the optimal dosage for children ages 5 to 11 to be one-third of the dose given to adults and adolescents and administered as a two-shot regimen three weeks apart.
No serious side effects related to the vaccine, and no cases of myocarditis were reported. The Pfizer data also showed that the vaccine in that age group seems to provide similar high levels of protective antibody responses to those seen in older age groups. And the antibodies produced demonstrated an ability to neutralize the delta variant.”
However, the number of children included in the clinical trials was relatively small compared to the clinical trials involving adults; in evaluation of safety and effectiveness data, there were fewer than 5,000 children each, in contrast to tens of thousands of people in the clinical trials involving adults. Therefore, continued monitoring of the vaccine post-authorization will enable health authorities to detect extremely rare side effects if there are any. Continued studies will also allow researchers to assess the longevity of vaccine-induced immunity in children.
While children do face a lower risk of illness, hospitalization, and death from COVID-19 compared to adults, overall these risks still exceed the risks posed by the COVID-19 vaccine. An elevated risk of myocarditis, a form of heart inflammation, has been associated with COVID-19 RNA vaccines, particularly in young boys and men[2]. However, COVID-19 itself is more likely to result in myocarditis[3], and a study by CDC researchers found that the benefits of the vaccine, in terms of COVID-19 cases, hospitalizations, and deaths avoided, far outweigh cases of myocarditis associated with the vaccine[4].
The American Academy of Pediatricians (AAP) recommends that children get vaccinated against COVID-19 if they’re eligible. Lee Savio Beers, the president of the AAP stated that “We know from our experience with the Delta variant that this virus is unpredictable, and we cannot afford to be complacent. It is critical to use science and data to guide our decisions about the pandemic and school COVID-19 plans.”
UPDATE (21 September 2022):
This review was updated to explain what the correct formula for NNTV should be.
REFERENCES
- 1 – Hashim et al. (2015) How and why researchers use the number needed to vaccinate to inform decision making—A systematic review. Vaccine.
- 2 – Mevorach et al. (2021) Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. New England Journal of Medicine.
- 3 – Boehmer et al. (2021) Association Between COVID-19 and Myocarditis Using Hospital-Based Administrative Data — United States, March 2020–January 2021. Mortality and Morbidity Weekly Report.
- 4 – Gargano et al. (2021) Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices — United States, June 2021. Mortality and Morbidity Weekly Report.
