

Misleading: Ryan implied that COVID-19 vaccines aren’t working because vaccinated people must still practice physical distancing and wear masks. This isn’t true. Because it is unclear how much the vaccines reduce transmission, vaccinated people need to practice physical distancing and wear masks to protect the unvaccinated people around them, who are the majority.
Unsupported: No reliable scientific evidence supports the claim that ivermectin is an effective treatment against COVID-19. Larger and better-designed studies are required to determine ivermectin’s effect on COVID-19 patients.

RECLAMACION: Coronaviruses are all seasonal and go away on their own, including those that cause SARS and MERS; ivermectin is effective for preventing and treating COVID-19; COVID-19 vaccines are “gene therapy”, don’t give immunity or prevent transmission
REVIEW
On 4 March 2021, pathologist Ryan Cole gave a speech to lawmakers at the Idaho State Capitol Building. Cole made several claims about the COVID-19 pandemic and vaccines, several of which were previously debunked by fact-checkers. His speech was uploaded to multiple platforms, including YouTube, Instagram, and Bitchute, and went viral. One copy on Instagram received more than 660,000 views, another on YouTube received more than 245,000 views, and yet another copy on Bitchute received more than 180,000 views.
This review explains below why several of Cole’s claims are inaccurate, misleading, or unsupported by scientific evidence.
Claim 1 (Inaccurate and Misleading):
“Coronaviruses are seasonal. They follow a six-to-nine-month life cycle, and no matter what we do, they’re going to do what they do, and then they’re going to fade. What happened to SARS, what happened to MERS? What did we do to stop them? Nothing, they did their thing.”
Disease seasonality refers to when the number of infections rise at certain times of the year, but are low at other times, and when the pattern repeats itself every year. This pattern is observed in several infectious diseases, including some common coronaviruses[1,2], but Cole’s claim seemed to imply that “a six-to-nine-month life cycle” is a rule for all coronaviruses. This is contradicted by the fact that more than a year later, COVID-19 is still actively spreading in several parts of the world, including the U.S. and European countries like France and Italy.
It is inaccurate and misleading to cite SARS (severe acute respiratory syndrome) and MERS (Middle East respiratory syndrome) as examples of diseases caused by seasonal coronaviruses. Neither of these viruses exhibit seasonal activity. The first outbreak of SARS began in 2003, with a second, smaller outbreak occurring in 2004 after researchers studying the SARS coronavirus became infected by accident. No other cases of SARS were recorded after that. If SARS was a seasonal disease, as Cole claimed, new cases would be expected each year.
MERS was first reported in 2002. Researchers studying the pattern of MERS cases between 2015 and 2017 concluded that the disease doesn’t exhibit seasonality, at least in terms of primary infections[3].
It is also false to claim that nothing was done to stop SARS and MERS. Unlike COVID-19, no community spread of SARS took place in the U.S.. As such, the country didn’t experience widespread cases of SARS. According to the U.S. Centers for Disease Control and Prevention (CDC), there were only eight cases of SARS-CoV-1 infection, all of which were linked to travel in areas where SARS was spreading. Given the fact that there was no community spread of SARS, no control measures were imposed on the general public.
This wasn’t the case for regions that saw SARS spread, including China, Singapore, and Hong Kong. All three countries implemented significant control measures to reduce the spread of SARS, such as temperature screenings, contact tracing, school closures, and implementing quarantines of contacts and suspected cases[4].
As with SARS, the U.S. didn’t see widespread transmission of MERS. The CDC reported that only two people in the U.S. tested positive for MERS, both in 2014. The global spread of MERS, like SARS, was largely confined to a specific geographic region, namely the Arabian Peninsula. One exception is South Korea, which saw an outbreak in 2014 that was linked to one traveller who visited the Middle East. That outbreak was brought under control thanks to public health measures, including contact tracing and quarantine and isolation of all contacts and suspected cases.
Overall, Cole’s suggestion that COVID-19 is a seasonal disease that will go away on its own in six to nine months, even if we don’t do anything, doesn’t stand up to scrutiny. It has been more than a year since the COVID-19 pandemic started. His claim that the coronaviruses responsible for SARS and MERS are seasonal and that nothing was required to control their spread is inaccurate.
Claim 2 (Misleading):
“90% of deaths in the state have been over 70 years of age. That’s the at-risk population. We have stopped our society for something that’s taking people that are already at that death risk age anyway”
Cole’s statements appear to reference the public health measures used to control the spread of COVID-19, including lockdowns and physical distancing. There have been numerous claims that attempt to downplay the severity of the COVID-19 pandemic by focusing on the disease mortality. Health Feedback reviewed some of these claims here and here.
This claim overlooks the fact that the outcomes of COVID-19 aren’t limited to either complete recovery or death. While most people who get COVID-19 survive, a certain proportion of survivors struggle with long-term health problems, which researchers termed “long COVID”. Among some of the documented effects are shortness of breath, fatigue, and an inability to focus or think clearly (“brain fog”). These effects can considerably affect a person’s quality of life.
Long COVID affects a wide variety of people, including those who had mild or serious COVID-19, as well as young, athletic, and elderly people. It is also unclear how long it will take for the effects to go away, as Stephanie LaVergne, an infectious disease researcher at Colorado State University, wrote in The Conversation.
Cole’s claim that 90% of deaths in Idaho came from those over 70 years of age isn’t accurate. According to the Idaho Department of Health and Welfare, those aged 70 years old and above comprise about 80% of COVID-19-related deaths (see Figure 1 below).
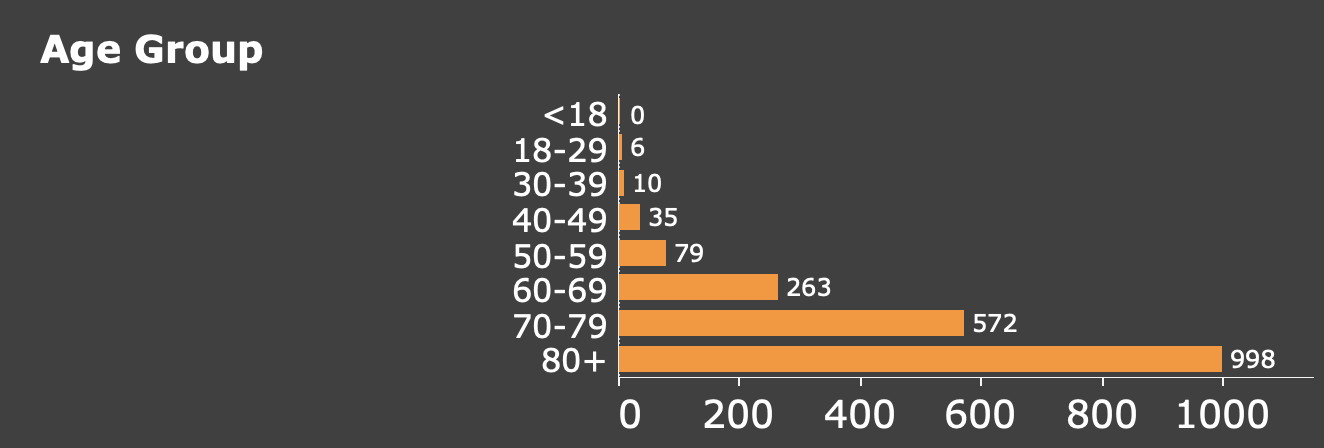
Figure 1. Number of COVID-19-related deaths in the state of Idaho, stratified by age. Data extracted on 2 April 2021 from the Idaho Division of Public Health.
Claim 3 (Unsupported):
Ivermectin is effective for preventing and treating COVID-19
Claims about ivermectin’s efficacy against COVID-19 circulated on social media even before Cole’s video. Health Feedback fact-checked the claim about ivermectin in previous reviews here and here.
Ivermectin is a drug used to treat parasitic infections in both animals and humans. The basis for the claim that the drug works on COVID-19 appears to come, at least in part, from a study by researchers in Australia that tested the drug in cells growing in Petri dishes[5]. They observed that ivermectin could reduce viral replication in cells infected by SARS-CoV-2. However, the dose used in this study was many times higher than doses approved for humans[6].
Researchers conducted clinical trials testing the effectiveness of ivermectin on COVID-19 patients. A summary of the results and limitations of some clinical studies on the effects of ivermectin on COVID-19 is available on the U.S. National Institutes of Health COVID-19 Treatment Guidelines website. As the website explained, several trials had limitations, which affected the strength of their conclusions, such as a small sample size, lack of clarity regarding the severity of COVID-19 in patients enrolled in the trials, and patients receiving multiple medications at the same time, making it difficult to determine what effects were due to ivermectin alone.
Because of the poor quality of evidence, the COVID-19 Treatment Guidelines Panel concluded:
“Because most of these studies have significant limitations, the Panel cannot draw definitive conclusions on the clinical efficacy of ivermectin for the treatment of COVID-19. Results from adequately powered, well-designed, and well-conducted clinical trials are needed to provide further guidance on the role of ivermectin in the treatment of COVID-19.”
Overall, there is no reliable scientific evidence for Cole’s claim that ivermectin is effective for treating COVID-19.
Claim 4 (Inaccurate and Misleading):
COVID-19 vaccines are “experimental biological gene therapy”; “mRNA trials in mammals have led to odd cancers, mRNA trials on mammals have led to autoimmune diseases”
Cole claimed that COVID-19 RNA vaccines are gene therapies. This is false. Gene therapies modify a person’s DNA in order to treat a disease. As explained in this Health Feedback review, RNA vaccines cannot modify DNA. As such, they cannot function as gene therapy.
Cole’s claim that RNA vaccine trials led to cancer and autoimmune diseases are unsubstantiated, as he didn’t provide any evidence for these claims.
Claim 5 (Inaccurate and Misleading):
“You know, do the shots decrease severity of disease and hospitalization? Well, they seem to be, but they don’t fall under the definition of creating pure immunity and preventing transmission. If you’re immune after an injection, why in the world would you still have to mask and social distance? That is an admission that they don’t know that it’s a vaccine.”
Although it’s unclear what Cole meant by “pure immunity”, the CDC defines the term “vaccine” as follows:
“A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease. Vaccines are usually administered through needle injections, but can also be administered by mouth or sprayed into the nose.” (emphasis added)
Given that the COVID-19 vaccines authorized for use by the U.S. Food and Drug Administration (FDA) all effectively reduced the likelihood of illness and severe disease, they induce immunity by the CDC’s definition.
And as Sarah Caddy, a clinical research fellow in viral immunology at the University of Cambridge, explained in this article published by The Conversation:
“In reality, it is actually extremely difficult to produce vaccines that stop virus infection altogether. Most vaccines that are in routine use today do not achieve this. For example, vaccines targeting rotavirus, a common cause of diarrhoea in infants, are only capable of preventing severe disease. But this has still proven invaluable in controlling the virus. In the US, there has been almost 90% fewer cases of rotavirus-associated hospital visits since the vaccine was introduced in 2006. A similar situation occurs with the current poliovirus vaccines, yet there is hope this virus could be eradicated globally.”
In short, there are many vaccines that induce immunity and produce benefits, even though they don’t stop virus infection completely.
Cole’s conclusion that “they don’t know that it’s a vaccine” because vaccinated people still need to wear a mask and practice physical distancing is misleading. A similar claim was previously fact-checked by Health Feedback and found to be misleading.
The reason why public health authorities recommend that vaccinated people wear face masks and practice physical distancing is because researchers haven’t yet determined how much the COVID-19 vaccines reduce virus transmission. While the evidence shows that vaccines effectively reduce the risk of disease, we still don’t know conclusively if vaccinated people can transmit the virus to unvaccinated people.
Overall, the recommendations for vaccinated people isn’t an indication that the vaccines don’t work. Rather, it is because unvaccinated people are likely to remain the majority in most countries for at least several months, since not everyone can be vaccinated at the same time. And in the absence of conclusive evidence on the vaccines’ ability to block transmission, public health authorities are exercising caution by urging vaccinated people to continue to wear face masks and practice physical distancing, to protect the unvaccinated majority.
Claim 6 (Misleading):
“But if you get a coronavirus shot, historically, SARS, MERS, animal coronaviruses […] when you’re exposed to a wild-type variant of the virus […] months later, the immune system can go haywire. In the SARS vaccine trials in the ferrets and the monkeys, 100% of the animals, when exposed to wild-type virus, ended up with immune reaction.”
Cole referred to a commonly repeated claim that the COVID-19 vaccines will lead to more severe disease. This is most likely a reference to the immunological phenomenon known as antibody-mediated enhancement (ADE). Health Feedback previously reviewed claims relating to ADE here and here.
ADE occurs when antibodies bind to a virus in a manner that fails to neutralize a virus’ infectivity, but instead makes it easier for the virus to infect cells. The potential danger posed by ADE is one that scientists developing vaccines are mindful of.
This is due to previous experiences with vaccine candidates for other coronaviruses, such as the virus SARS-CoV-1, which causes SARS, as well as coronaviruses that infect animals. Researchers developed a vaccine candidate for SARS-CoV-1 using inactivated (“killed”) virus, which was tested in mice. They observed that vaccinated mice showed more severe lung disease upon infection with live virus[7]. In the case of another coronavirus, cats that were vaccinated with a recombinant virus vaccine survived for a shorter period of time compared to unvaccinated cats[8].
A vaccine candidate against the respiratory syncytial virus (RSV) also failed human clinical trials, as it caused more severe illness in vaccinated people[9].
Because these studies highlighted the problem of ADE from vaccines, researchers are aware that this is a potential risk of COVID-19 vaccines that needs to be monitored. The vaccines authorized for emergency use by the FDA are carefully monitored for ADE and other severe side effects.
Indeed, clinical trials didn’t show any indication that ADE occurs in people who received the COVID-19 vaccines. Walter Orenstein, a professor at Emory University’s School of Medicine and associate director of the Emory Vaccine Center, stated in this Health Feedback review: “Vaccine-enhanced disease is theoretically possible with SARS-CoV-2 vaccines, but it has not been seen as of yet in the clinical trials reported.”
READ MORE
Chief medical officer at St. Luke’s Hospital James Souza fact-checked some of Cole’s claims; his comments can be seen in this video.
