

BEHAUPTUNG: “SARS-CoV-2 vaccination was associated with higher risk of myocarditis death”; “we conclude that the high association of high myocarditis mortality rate ratios after SARS-CoV-2 vaccination may be causal”; “This study published Oct 19th 2022 shows that if you inject new technology filled with highly toxic materials like polyethylene glycol and graphene oxide into your body then the body with (sic) have an inflammatory response.”
REVIEW
A preprint (a study that hasn’t been peer-reviewed yet), uploaded to the server medRxiv, claimed that relative to pre-pandemic years, “SARS-CoV-2 vaccination was associated with higher risk of myocarditis death, not only in young adults but also in all age groups”.
The researchers arrived at this conclusion by comparing mortality data from pre-pandemic years and data on post-vaccination deaths released by Japan’s Ministry of Health, Labor, and Welfare on 5 August 2022. The researchers used the data to calculate what they called the “myocarditis mortality rate ratio” (MMRR) and reported an elevated MMRR in all age groups, with the rate being almost seven times higher in young adults when compared to the same age group in pre-pandemic times.
Outlets that included The Epoch Times, New Tang Dynasty (run by the same company that owns The Epoch Times), and Children’s Health Defense served as a springboard for the preprint’s claims on social media. A screenshot of the preprint was also shared on Instagram by chiropractor Stephen Hussey, who has more than 23,000 followers.
In addition to the screenshot, Hussey claimed that the study showed what happens “if you inject new technology filled with highly toxic materials like polyethylene glycol and graphene oxide into your body”. This is a rehash of pre-existing false information about COVID-19 mRNA vaccines. Firstly, graphene oxide isn’t present in COVID-19 vaccines. Secondly, polyethylene glycol, an ingredient found in the COVID-19 mRNA vaccines, isn’t toxic at the levels that are used in the vaccines.
More importantly, the data collected and analyzed in the preprint don’t provide sufficient evidence for the authors’ conclusions regarding harm from the COVID-19 vaccines, and by extension, the claim propagated by The Epoch Times and other websites on social media.
Firstly, post-vaccine myocarditis deaths were defined as deaths in which the signs and symptoms of myocarditis occurred within 28 days of the last COVID-19 vaccine dose. The authors attributed deaths to myocarditis based on autopsy results or post-mortem biopsy results.
However, there’s no indication that the authors examined the medical histories of the people who died of myocarditis. This would have made it impossible for them to account for other plausible causes of myocarditis, notably COVID-19[1], another viral infection or an autoimmune disease.
Secondly, the authors’ association of change in the risk of myocarditis death associated with COVID-19 vaccines was based on comparing pre-pandemic and post-pandemic rates of myocarditis death.
But this assumes that the only thing that changed between the two periods is the availability of the COVID-19 vaccines. It excludes, without justification, the possibility that COVID-19 itself could produce an increase in myocarditis deaths. No reason was given by the authors for excluding COVID-19 as a potential explanation, despite the fact that COVID-19 is a more likely explanation than COVID-19 vaccines for an increase.
This is because we know—based on previous published studies—that COVID-19 is more likely to lead to cardiac complications than the vaccines[2,3]. Therefore, the alleged causal association rests on the assumption that only COVID-19 vaccines can explain the change in myocarditis mortality, which isn’t true.
The American Heart Association considers the benefits of the COVID-19 vaccines to outweigh their risks. An expert consensus by the American College of Cardiology also found that “a very favorable benefit-to-risk ratio exists with the COVID-19 vaccine for all age and sex groups evaluated thus far”[4].
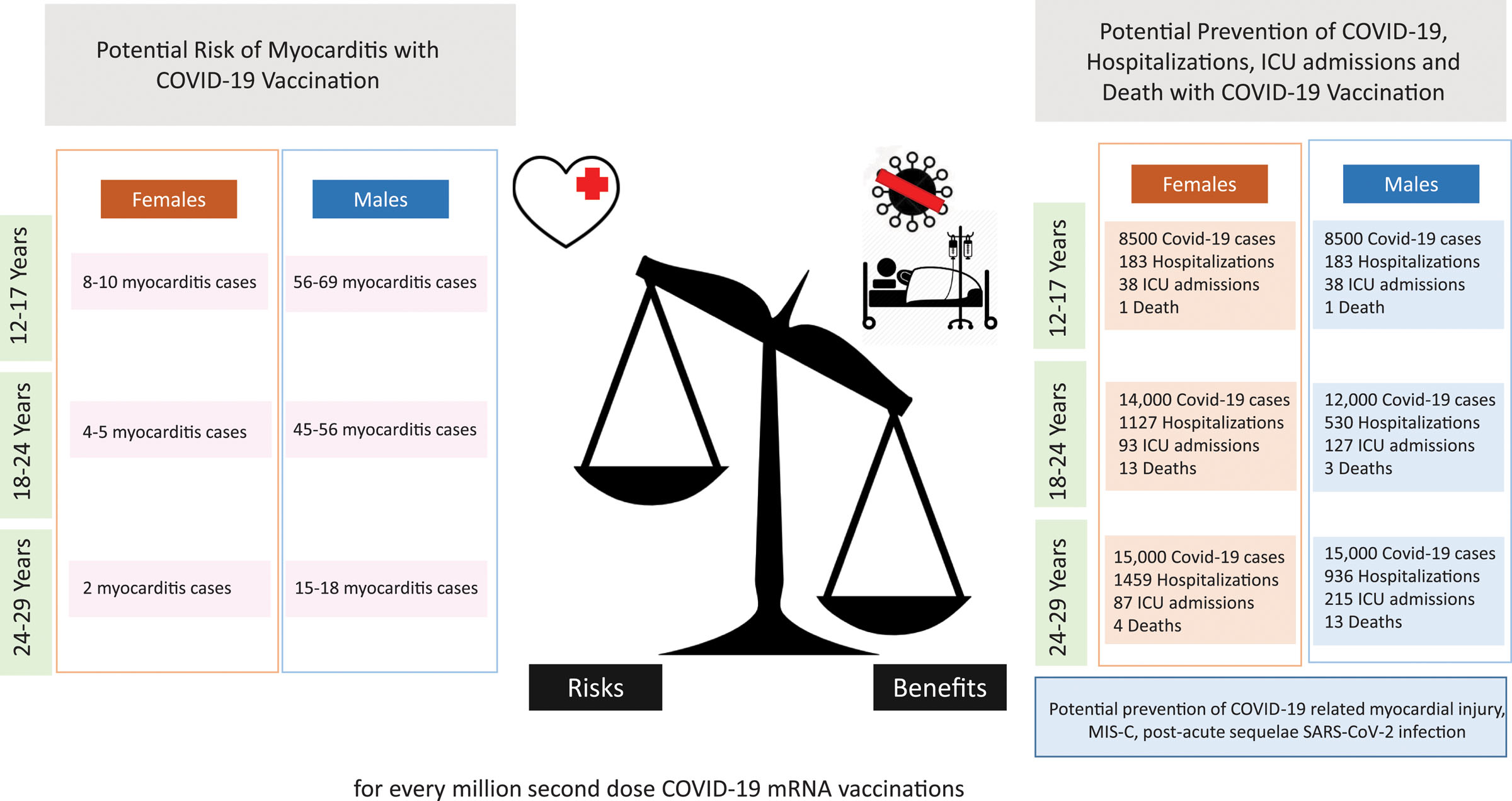
Figure 1. There is a favorable benefit-to-risk ratio for COVID-19 mRNA vaccine recipients at highest risk for postvaccination myocarditis[5]. The predictions for hospitalization and myocarditis rates were calculated for every million doses of mRNA vaccine, based on the hospitalization rates from Coronavirus Disease 2019 (COVID-19)–Associated Hospitalization Surveillance Network (COVID-NET) as of May 2022. Benefit/risk were calculated over 120 days.
Thirdly, the study only included 38 post-vaccine myocarditis deaths in its analysis (out of 1,362 all-cause deaths). In its attempt to establish MMRR by age group, we can see that there are very few deaths in each group—none reached double digits and certain groups had no myocarditis deaths at all (Table 1). This is in contrast to the pre-pandemic data analyzed by the authors, which included more than four million all-cause deaths and more than 400 myocarditis deaths.
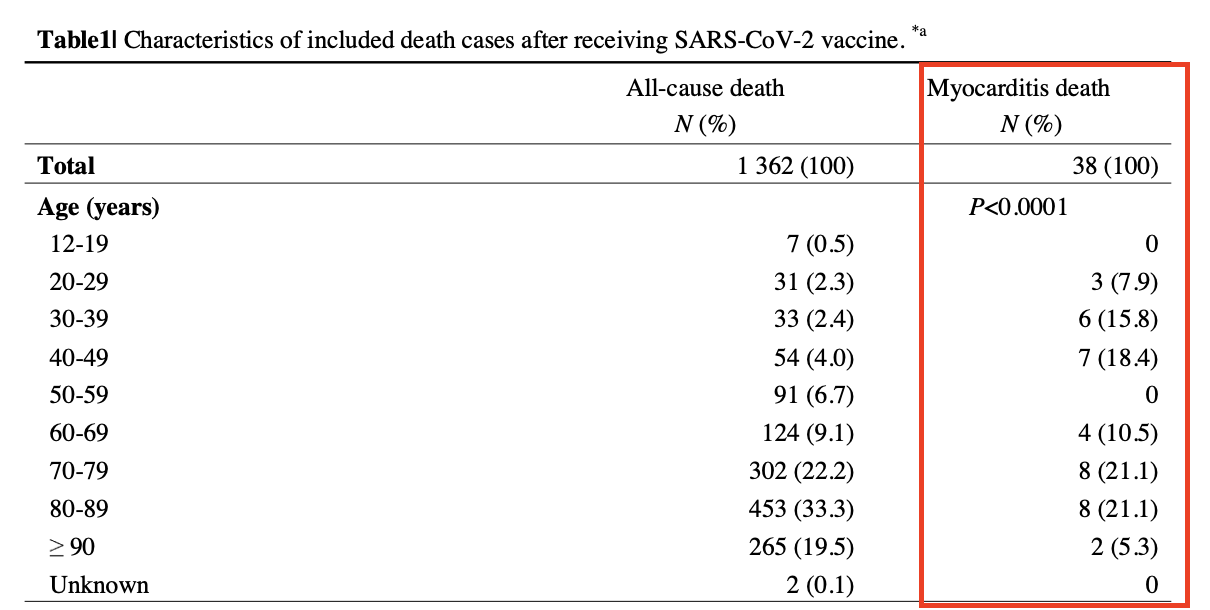
Table 1. The preprint included 1,362 deaths from any cause 28 days following vaccination. Among these, 38 were deaths from myocarditis. In certain age groups, no myocarditis deaths were recorded.
The small sample size analyzed—coupled with the even smaller numbers when divided into sub-groups—makes it difficult for us to ascertain whether the association that the authors reported is the result of a genuine effect or simply a statistical fluke due to the low statistical power.
Overall, the claim that this preprint showed COVID-19 vaccination to carry a higher myocarditis risk than expected is unsubstantiated by the work actually performed by the preprint authors. The authors failed to account for other causes of myocarditis apart from the COVID-19 vaccines without justification. The sample size analyzed was also small, which casts doubt over whether the alleged causal association is the result of a genuine effect or simply a statistical fluke. Larger, more reliable studies have shown that the benefits of the COVID-19 vaccines outweigh their risks, even in those groups at the highest risk of post-vaccine myocarditis.
REFERENCES
- 1 – Boehmer et al. (2021) Association Between COVID-19 and Myocarditis Using Hospital-Based Administrative Data — United States, March 2020–January 2021. Mortality and Morbidity Weekly Report.
- 2 – Block et al. (2022) Cardiac Complications After SARS-CoV-2 Infection and mRNA COVID-19 Vaccination — PCORnet, United States, January 2021–January 2022. Mortality and Morbidity Weekly Report.
- 3 – Patone et al. (2022) Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation.
- 4 – Writing Committee. (2022) 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology.
- 5 – Bozkurt et al. (2021) Myocarditis With COVID-19 mRNA Vaccines. Circulation.
