

Misleading: The comparison between the current fatality rate of the Delta variant with the fatality rate of the wild-type virus prior to the U.K. vaccination campaign is flawed. The fatality rate of the Delta variant mainly represents that of the unvaccinated population, most of whom are under 50 years old and are less likely to die from COVID-19.

AFFIRMATION COMPLETE: The fatality rate of the Delta variant of COVID-19 is lower than the original variant. The latest data from the U.K. shows the case fatality rate for the Delta variant amongst the unvaccinated is 0.08%, which makes it less deadly that the normal flu. This Delta variant is one-tenth as deadly as the wild-type virus.
REVIEW
Different variants of the SARS-CoV-2 virus, which causes COVID-19, have emerged throughout 2020 and 2021. Certain kinds of mutations make each variant genetically distinct from the precursor (wild-type) virus and from each other. These genetic differences can alter the transmissibility of the virus, the severity of the symptoms of the disease and/or the effectiveness of vaccines.
One variant of concern, first identified in India in December 2020, is the Delta variant or B.1.617.2. This variant has distinctive mutations that could increase its infectivity, being more contagious than other variants and than the wild-type virus. The Delta variant has spread in several countries, including the U.K., where it is already the predominant variant of the virus.
On 4 July 2021, American radio broadcaster Dan Bongino published a video on Facebook in which he questioned the lethality of this variant, claiming that it was less deadly than the original variant. The video received more than 20,000 interactions on Facebook according to social media analytics tool CrowdTangle.
In support of this claim, the video included a clip of a Sky News Australia interview with Australian Member of Parliament Craig Kelly conducted on 1 July 2021 by Alan Jones. In this interview, Jones referred to epidemiological data on the Delta variant in the U.K., stating that its case fatality rate was 0.08% among the unvaccinated population, and therefore it would be less lethal than the normal flu. Kelly added that the Delta variant has one-tenth the lethality of the wild-type virus.
These statements are inaccurate and misleading, as they are based solely on the fatality rate in the unvaccinated population in the U.K., who are mostly people under 50 years old who don’t belong to risk groups.. Therefore, the fatality rate for the unvaccinated population doesn’t reflect the threat posed by the virus on the population as a whole. This review discusses the current data available on the case fatality rate of the Delta variant of SARS-CoV-2, and how age and the current vaccination campaign affect the case fatality rate.
The COVID-19 vaccination campaign in the U.K. prioritized groups at a higher risk of dying from COVID-19, such as older age groups; vaccination now protects these groups
The COVID-19 vaccination campaign in the U.K. started in December 2020. This vaccination campaign was carried out by dividing the population into priority groups, based on age and the presence of underlying clinical conditions. A significant percentage of the population over 18 years of age has already received at least one dose of the vaccine as of 24 june 2021, according to a report from Public Health England (see Figure 1).
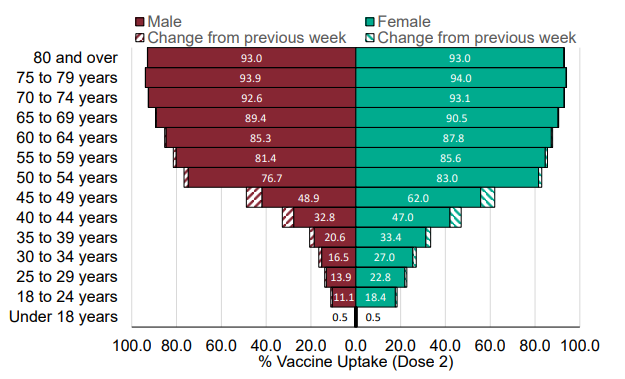
Figure 1. Age/Sex pyramid for COVID-19 vaccine uptake by age in England for dose 2, as of 24 June 2021. Source: Weekly national Influenza and COVID-19 surveillance report. Week 26 report (up to week 25 data), 1 July 2021. Public Health England.
According to an analysis by the BBC published on 6 July 2021, “Wales has vaccinated 90% of those aged 18 and over with at least one dose, while Scotland has reached 86%, England 85% and Northern Ireland 80%. Second doses are also being rolled out, with all nations reaching 60% or more of adults so far”.
Also, according to estimates from Public Health England, the vaccination campaign in the U.K. prevented between 6.4 and 7.9 million cases of COVID-19 and between 26,000 and 28,000 deaths until 27 June 2021. It has also been estimated that around 44,500 hospitalizations were prevented in those aged 65 and older.
Most cases of Delta variant infection are in unvaccinated people, who are younger than 50 years old and less likely to die from COVID-19; the Delta variant CFR may therefore be an underestimate
The U.K. is the country with both the highest number of cases and the highest prevalence of the Delta variant as of 5 July 2021, according to the open-access genomic database GISAID. GISAID is officially recognized by the European Commission as a research organization and partner in the PREDEMICS consortium, which works on pandemic preparedness.
The Delta variant was detected for the first time in the U.K. in February 2021. Based on the number of COVID-19 cases in which the virus was identified by genetic sequencing, the prevalence of the Delta variant in the country began to rise in May 2021, as shown in Figure 2. By June 2021, the Delta variant represented 97.8% of all cases of COVID-19 in the U.K.
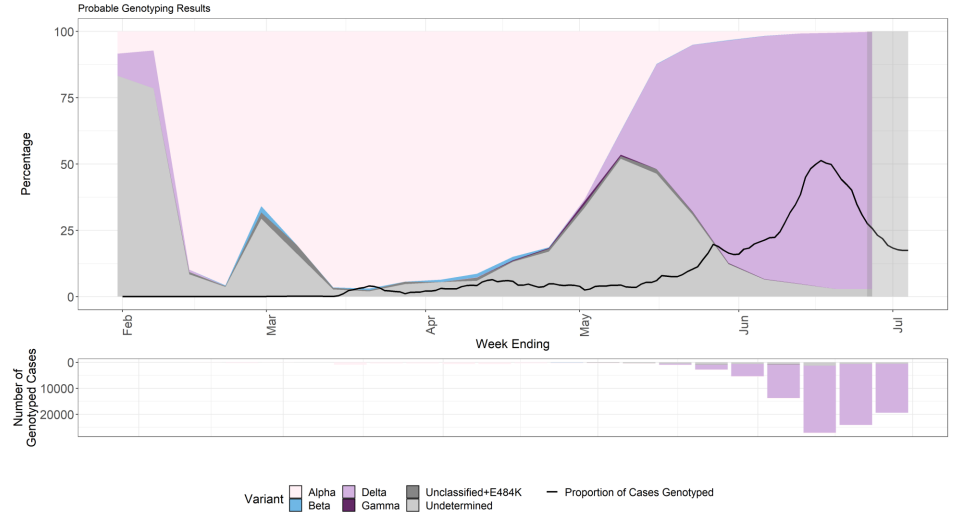
Figure 2. Prevalence of each variant in all of England, based on genotyped cases from 1 February to 5 July 2021. Source: SARS-CoV-2 variants of concern and variants under investigation in England. Technical Briefing 18, 9 July 2021. Public Health England.
According to a report on SARS-CoV-2 variants of concern in England, published by Public Health England on 9 Jul7 2021, as of 5 July 2021, 123,620 COVID-19 cases were caused by the Delta variant in England. The case fatality rate (CFR) for the Delta variant in the general population is 0.2%, according to the report. The CFR is the proportion of cases of a disease that end in death, among all diagnosed cases.
It’s important to note that the CFR figures reported may underestimate the fatality rate of the Delta variant, due to a delay in reporting deaths. This caveat is indicated in a previous report from Public Health England, published 11 June 2021, “the 28-day case fatality rate for Delta remains low (0.1%), though mortality is a lagged indicator and the vast majority of cases are still within the 28 days of follow-up required”.
In addition, context is important when interpreting the data. According to the same report, in the population aged 50 years or older, 12,404 COVID-19 cases by the Delta variant were detected between 1 February and 21 June 2021, of which 231 died, resulting in a CFR of 1.9% for this age group. At the same time, 111,008 COVID-19 cases caused by the Delta variant were detected in people under 50 years old in the U.K., of which 26 died, giving a CFR of 0.02% for this age group. This is, 90% of cases of COVID-19 by the Delta variant occurred among the population under 50 years old, and just 10% of cases among the population aged 50 or older.
Another factor that must be taken into account when interpreting the data is that the majority of COVID-19 cases caused by the Delta variant are recent, with 52% of new cases reported in the population under 50 years old in the 28 days prior to 21 June 2021, and 48% of new cases reported in the population aged 50 years or older in the same period.
Research done in a number of countries throughout the pandemic has shown that age plays a role in the CFR of COVID-19. A study based on surveillance data carried out in Italy at the beginning of the pandemic reported that the CFR was higher in the older population. The CFR in the age group under 50 years old was less than 1. But this more than doubled in the 50-59 age group, with a CFR of 2.5, further increasing as age groups became older. Despite the limitations of this study acknowledged by the authors, related to under-notification of cases, these results show how age increases risk for death from COVID-19[1].
Another study, conducted in 20 European countries, Canada, and the U.S., found that variation in the COVID-19 CFR was related to the proportion of people over 75 years old diagnosed with the disease, with the CFR increasing by 2.5% for every 5% increase in the representation of this age group among the diagnosed cases[2]. These results show how the CFR of COVID-19 is highly dependent on the age of the infected individuals. The higher the age of the infected individuals, the higher the CFR, and vice versa.
As explained earlier, vaccines have considerably reduced the number of COVID-19 deaths in recent months and are highly effective. Given that the Delta variant in the U.K. is growing more prevalent at a time when many people are already vaccinated and therefore less likely to become ill and die, comparing the fatality rate of the Delta variant with the fatality rate of the virus before the protection afforded by COVID-19 vaccines was widely available is misleading, as most of the people who are at greater risk of dying from COVID-19 have already been vaccinated.
The existing data don’t allow us to conclude that the Delta variant has a lower CFR than the wild-type virus. Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security, explained in a PolitiFact fact-check that “All variants are going to have a lower case fatality rate, because a significant portion of the population, especially those at high risk for death, are fully or partially vaccinated”.
However, an increase in hospitalizations due to the Delta variant has been reported in the U.K., while in Scotland, the risk of hospitalization for the Delta variant was found to be twice as high as for the Alpha variant, which was the predominant variant in the U.K. previously[3], suggesting that the Delta variant could be more likely to cause serious illness.
The claim that the CFR of the Delta variant is 0.08% is misleading, as this value varies greatly depending on the age of the population and its vaccination status. To put this in context, according to the latest Public Health England report, the CFR for the Delta variant is 1.9% for people over 50 years old. The video published by Dan Bongino didn’t explain this, leaving viewers with the false impression that the Delta variant is less deadly than the wild-type virus.
Finally, the comparison of the CFR of the Delta variant with the CFR of flu is flawed. As explained above, the CFR of the Delta variant isn’t representative of the entire population, as most cases of Delta variant infection are in people under 50 years old. As with COVID-19, the fatality rate of flu varies greatly depending on age, so comparing the overall CFR of flu with the CFR of the Delta variant, which is primarily derived from a younger population, is flawed[4].
Conclusion
The CFR of the Delta variant is low for the general population, around 0.2%, but this may be because most of the population at a higher risk of dying from COVID-19 has been vaccinated in the U.K., which has reduced deaths caused by the disease. This also means that those who remain unvaccinated and unprotected are mainly people under 50 years old. The majority of Delta variant infections in the U.K. are occurring in this population, hence the CFR of the Delta variant mainly represents that of the population under 50 years old. Comparing the CFR of the Delta variant with that of the wild-type virus at a time before vaccines were available is misleading, since the former excludes most of the population over 50 years old, which has a higher CFR but is mostly vaccinated. In summary, there isn’t sufficient evidence that allows us to conclude that the Delta variant of SARS-CoV-2 is less lethal than the wild-type virus.
UPDATE (12 July 2021):
This review was updated to clarify why Bongino’s claim that “the CFR of the Delta variant is 0.08%” is misleading.
REFERENCES
- 1 – Signorelli and Odone (2020) Age-specific COVID-19 case-fatality rate: no evidence of changes over time. International Journal of Public Health.
- 2 – Hoffman and Wolf (2021) Older age groups and country-specific case fatality rates of COVID-19 in Europe, USA and Canada. Infection.
- 3 – Sheikh et al. (2021) SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness. The Lancet.
- 4 – Wong et al. (2013) Case fatality risk of influenza A(H1N1pdm09): a systematic review. Epidemiology.
