- Health
Video shared by Sebastian Gorka Facebook page shows nurse making false and unsubstantiated claims about ivermectin, COVID-19 PCR tests, and COVID-19 vaccine safety
Key takeaway
Data from clinical trials and ongoing monitoring of vaccination campaigns show that COVID-19 vaccines are very safe and effective. Their benefits outweigh their risks, as they are highly effective at reducing a person’s risk of infection and severe illness. There is no reliable scientific evidence demonstrating that ivermectin is an effective COVID-19 treatment, although research is currently underway to resolve this question.
Reviewed content
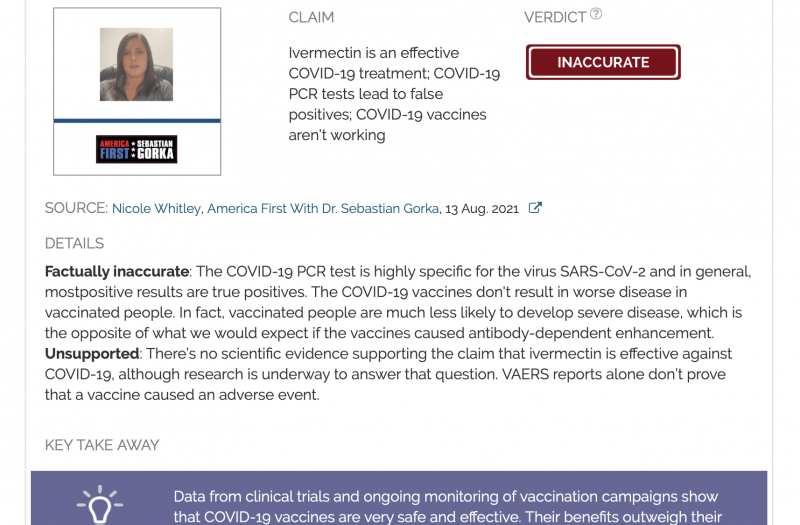
Verdict:
Claim:
Ivermectin is an effective COVID-19 treatment; COVID-19 PCR tests lead to false positives; COVID-19 vaccines aren’t working
Verdict detail
Factually inaccurate: The COVID-19 PCR test is highly specific for the virus SARS-CoV-2 and in general, mostpositive results are true positives. The COVID-19 vaccines don't result in worse disease in vaccinated people. In fact, vaccinated people are much less likely to develop severe disease, which is the opposite of what we would expect if the vaccines caused antibody-dependent enhancement.
Unsupported: There’s no scientific evidence supporting the claim that ivermectin is effective against COVID-19, although research is underway to answer that question. VAERS reports alone don’t prove that a vaccine caused an adverse event.
Full Claim
Ivermectin is an effective COVID-19 treatment; COVID-19 PCR tests lead to false positives; animals died from antibody-dependent enhancement during SARS-CoV-1 vaccine trial; COVID-19 vaccines aren’t working; data from Israel and Australia show COVID-19 vaccines aren’t working; VAERS reports show that COVID-19 vaccines are unsafe
Review
On 13 August 2021, the Facebook page “America First With Dr. Sebastian Gorka” published a video of nurse Nicole Whitley, who made several claims about ivermectin, COVID-19 vaccine safety, and the COVID-19 PCR tests. Sebastian Gorka is a military and intelligence analyst who served as Deputy Assistant to the President during the Trump administration.
The video was also shared on Rumble by a channel bearing the same name as the Facebook group and on Instagram by mixed martial artist Mitch Aguiar. All in all, copies of the video received more than 2 million views.
The claims made by Whitley were debunked in earlier fact-checks by both Health Feedback and other fact-checkers, as we show below.
Claim 1 (Unsupported):
“We have a drug [ivermectin] that is safe, it is cheap, it is highly effective, and it is widely available, and it’s not being used. There is no other medication to treat COVID that has simultaneously shown impacts on the prevention of transmission, viral clearance, which is how long it takes your body to get rid of the virus, the time to clinical recovery, and the survival rates.“
This claim isn’t supported by the evidence from clinical trials which tested the effectiveness of ivermectin against COVID-19, whether as a preventative or a treatment. As Health Feedback explained in several reviews in the past (see here, here, and here), the current state of understanding about ivermectin’s effectiveness is poor. This is because the studies on this subject are limited in what they can tell us, due to issues such as small sample sizes and the absence of placebo controls.
At one point, Whitley showed a figure from a published article by Kory et al. in the American Journal of Therapeutics (Figure 6 to be precise)[1]. The figure showed the number of COVID-19 cases and deaths in Peruvian states, classified according to whether the state widely distributed ivermectin. Whitney held it up as an example of ivermectin’s effectiveness.
However, this is a purely correlative observation, and correlation alone doesn’t mean that there is a causal relationship between the two. Whitley failed to account for other factors that could also influence COVID-19 cases and deaths, such as the implementation of public health measures like lockdowns, mask-wearing, and physical distancing.
Whitley also cited a meta-analysis by another scientist named Tess Lawrie as supporting evidence for her claim, most likely this one. A meta-analysis is a study that systematically analyzes data from other studies on a particular subject in order to come to a conclusion about a scientific question. One of the strengths of meta-analyses lies in their greater statistical power. However, the reliability of their conclusions is determined by the quality of the studies that the author chooses to include—or it would simply be a case of “garbage in, garbage out”.
As an earlier Health Feedback review explained, there are several issues with Lawrie’s analysis. For instance, it included a preprint (a study that hasn’t been peer-reviewed yet) by Elgazzar et al., which was later withdrawn for plagiarism and potential data fabrication. Another example is its presentation of clinical trials which obtained inconclusive results as supporting evidence for ivermectin’s effectiveness.
Due to the lack of evidence demonstrating the effectiveness of ivermectin, the U.S. National Institutes of Health COVID-19 Treatment Guidelines doesn’t recommend the use of ivermectin for treating COVID-19. The World Health Organization (WHO) also doesn’t recommend ivermectin as a COVID-19 treatment, except in clinical trials investigating its effectiveness. The question of ivermectin’s effectiveness is still an open one at the moment.
Claim 2 (Misrepresents source and Inaccurate):
“So, the PCR test, the way that they’re done, like I said, is a sensitivity test where they can set the cycle thresholds in order to detect the presence or absence of a virus. The creator of the PCR test said that this is not a diagnostic test and that they should not be used for that and yet, they were. And so, what we’re seeing, you know, in the beginning, we were seeing all these false positives.“
The claim that the COVID-19 PCR test is unreliable is popular in COVID-19 skeptic circles, commonly associated with anti-lockdown and anti-mask sentiments. Those who oppose these measures seek to discredit the PCR test since testing is linked to case numbers, which dictate the implementation of public health measures such as lockdowns and mask-wearing. By claiming that the test produces mainly false-positive results, they have grounds to claim that lockdowns and masks are unnecessary.
The claim that the PCR test produces largely false positives was addressed in earlier Health Feedback reviews here and here. As those reviews showed, the claim wrongly conflates infection and contagiousness. The COVID-19 PCR test detects the presence of genetic material from the virus SARS-CoV-2. It is highly sensitive and specific, meaning that it can detect very small amounts of genetic material and detects only genetic material from SARS-CoV-2.
The test can detect trace amounts of genetic material because it amplifies (makes many copies) of the viral genetic material. Cycle threshold (Ct) is the number of amplification cycles needed to arrive at a level considered to be a “positive” result. If the test detects the virus at a Ct of 30, it means that it took 30 amplification cycles to detect the virus. If it does so at a Ct of 25, then it took 25 cycles to reach the same threshold. The more genetic material in the sample, the fewer amplification cycles are needed to reach the same threshold.
The claim suggests that positive results with a high Ct are false positives. This is incorrect. A false-positive result occurs when a person who doesn’t have the infection tests positive. One possible cause is a contamination of the sample with virus from other samples during sample handling.
But samples that test positive with a high Ct simply indicate that a person harbors trace amounts of the virus, such as recovering patients. They are less likely to be contagious, but given that they were infected, it is still correct to consider them a case. The test cannot amplify genetic material that isn’t there and it doesn’t amplify genetic material from other viruses.
Kary Mullis, who received the Nobel Prize for inventing PCR, didn’t say that the test couldn’t be used for diagnosis. This is a popular but inaccurate claim that arose through a misinterpretation of statements made by Mullis about HIV patients. A quote from Mullis associated with this claim is “If they could find this virus in you at all, with PCR, if you do it well, you can find almost anything in anybody, it starts making you believe in the Buddhist notion that everything is contained in everything else.”
As explained in this fact-check by The Journal.ie, an Irish Internet publication, the claim left out the fact that in that quote, “Mullis was specifically discussing HIV and the experience of people with HIV who also contract other viruses”.
As explained by epidemiologist Gideon Meyerowitz-Katz in this article, “most positive coronavirus tests are true positives”.
Claim 3 (Misrepresents source and Inaccurate):
“[O]n January 20th, which is inauguration day, the World Health Organization instructed all of the labs to lower the cycle threshold and decrease the sensitivity“
The WHO did no such thing. The claim is based on a misinterpretation of a WHO information notice issued on 20 January 2021. As a blog post by virologist Ian Mackay explained, the notice was a reminder to laboratory staff to “Read the instructions and understand the purpose of testing”. Simply reading the information notice itself makes it evident that it contains nothing about lowering the cycle threshold or decreasing the test’s sensitivity. An earlier Health Feedback review debunked the claim.
Claim 4 (Inaccurate and Misleading):
“When they tried to use this technology to develop a vaccine for SARS CoV-1, what they found was that all of the animals, you know, they vaccinated them and they had a period of immunity and then, after that, when they were re-exposed to the virus, they all died. They attribute that to a condition which is known as antibody dependent enhancement.“
Claims about antibody-dependent enhancement (ADE) in the past have sometimes cited animal studies involving SARS-CoV-1 vaccine candidates. Antibody-dependent enhancement occurs when antibodies that bind to a disease-causing microorganism don’t mitigate illness, but exacerbate it instead.
It is unclear which study Whitley is referring to, but a study on vaccinated mice was previously cited in one such claim[2], which was debunked by Reuters. The lead author of the study refuted the claim, stating that the animals didn’t die after being vaccinated and didn’t show signs of illness, although they exhibited eosinophilia in the lungs. Eosinophilia means that there is a high level of eosinophils, a type of white blood cell.
Another possible study is this one conducted by researchers in China, which evaluated the efficacy of a SARS-CoV-1 vaccine candidate in ferrets[3]. But as is evident from reading the study itself, while the researchers did find signs of liver inflammation in the vaccinated ferrets that were exposed to the virus, which was hypothesized to be due to antibody-dependent enhancement, the animals displayed no sign of illness after vaccination.
The animals did die by the end of both studies, but this is because they had to be euthanized for researchers to collect tissue samples for testing. Claiming that the vaccines killed the animals misrepresents both studies.
There’s no indication that COVID-19 vaccines cause ADE. In fact, vaccinated people are much less likely to develop severe disease, which is the opposite of what we would get if the vaccines did cause ADE.
Claim 5 (Misrepresents source and Lacks context):
“[A]s we are hitting, you know, six months, eight months into our vaccination campaign, we are hearing now that all of these breakthrough cases are happening“
As supporting evidence for her claim, Whitley showed a NewsWars article bearing the headline “Israel, Australia report 95-99% of hospitalized fully vaccinated”. NewsWars is a website run by conspiracy theorist Alex Jones, who propagated false claims about a variety of subjects, ranging from the 2012 Sandy Hook Elementary School shooting to vaccine safety.
That article’s headline is a reference to a tweet sharing a news interview from Israel by physician Kobi Haviv at the Herzog Hospital, purportedly showing that 85 to 90% of hospitalizations for COVID-19 are in fully vaccinated patients, as well as an announcement from health official Jeremy McAnulty in New South Wales, Sydney on 25 July 2021, in which he stated that “all but one” of 43 COVID-19 patients in the ICU were vaccinated.
In the case of the 25 July 2021 press conference in New South Wales, McAnulty acknowledged in the same conference that he misspoke, after a journalist asked him to clarify his earlier statement. As this AAP fact-check pointed out, McAnulty corrected his mistake (see video at the 36:09 mark), saying “So of the 43 people in intensive care units, 42 have not been vaccinated. One person had just one dose of vaccine – incomplete vaccine”.
It is true that Israel, which launched one of the fastest COVID-19 vaccination campaigns in the world, is now seeing a rise in cases and hospitalizations due to the Delta variant. Because no vaccine is 100% effective, some infections still occur in vaccinated people. While reports from Israel, like this one in the Times of Israel, suggest that the vaccine’s effectiveness at preventing infection has waned in the face of the Delta variant, the vaccine still remains highly effective (>90%) at preventing serious illness.
Furthermore, the NewsWars article didn’t tell readers that in the Israeli news report, Haviv specified that most of the hospitalizations were in the elderly. And as the Times of Israel reported on 10 August 2021, the elderly population has the highest vaccine coverage in Israel:
“Nationally, some 90.2% of Israelis age 90-plus are vaccinated with at least two shots, and for the 80-89 age group the figure is 91.5%. It is even higher, 93.1%, for people in their 70s. But the rates decline among younger age groups: 87.2% for people in their 60s; 84.6 for people in their 50s and 81.2% for people in their 40s.“
This tells us that an overwhelming majority of the elderly (over 90%) is fully vaccinated. And when the vast majority of a group is vaccinated, one would expect that most, if not all, infections in that group will occur in vaccinated people. Put another way, if 100% of a group is vaccinated, any infections in that group must be in vaccinated people.
This doesn’t mean that the vaccine isn’t working. Indeed, all else being equal, vaccinated people are less likely to become ill and require hospital care compared to unvaccinated people. It is by thus comparing outcomes between vaccinated and unvaccinated groups that vaccine effectiveness becomes apparent, as this Financial Times article illustrated.
Claim 6 (Misleading):
“So currently in VAERS there are over 12,000 reports of death […] there’s 121 thousand reports of anaphylaxis. Over 8,000 reports of blood clotting disorders […] and over 2,000 cases of myocarditis and pericarditis. They’re seeing Guillain-Barré syndrome. They’re seeing Bell’s palsy, all sorts of neurological disturbances, seizures, 2,600 pregnant women have reported adverse events […] I find it criminal that they are doing this to kids, and I cannot help but wonder how much collateral damage we are willing to allow when we have safe and effective alternatives“
The overall implication of this claim is that adverse event reports submitted to VAERS are an indication that the COVID-19 vaccines are unsafe. This claim is popular in anti-vaccine circles and it has been covered in multiple news outlets, including NPR, Science Magazine, Global News, Vice, ABC News.
In brief, this claim is a misuse of VAERS data. Adverse event reports alone don’t prove that the vaccine was the cause. While thousands of reports were submitted, this should be viewed in light of the fact that to date, nearly two hundred million people in the U.S. have received at least one dose of COVID-19 vaccine.
When dealing with such a large population, incidental illnesses and deaths are a potential confounding factor, since people have been falling ill and dying even before COVID-19 vaccines were available. As explained in this Health Feedback Insight article, before hypothesizing a causal relationship between the vaccine and an adverse event, it is necessary to determine if the adverse event is occurring at a higher rate compared to the baseline or background rate of that event.
Overall, the benefits of the COVID-19 vaccines outweigh their risks. It’s unclear what “safe and effective alternatives” Whitley is referring to, but at the moment, there is no other clinically proven preventative for COVID-19 apart from vaccination.
Claim 7 (Inaccurate):
“When they brought the vaccines over to Japan, they wanted to do their own bio-distribution studies […] in this Japanese study, they found that across a period of time that [lipid nanoparticles are] heavily deposited in the spleen, the liver, the brain, the heart, the bone marrow, breast milk and particularly heavily in the ovaries”
This claim was made earlier by immunologist Byram Bridle. As explained in earlier Health Feedback reviews here and here, this is a misrepresentation of the biodistribution data.
To recap, Bridle claimed that the COVID-19 vaccines led to an accumulation of spike protein in various organs like the ovaries, which could cause damage to tissues. His claim was based on a few studies, including one by the Salk Institute[4], which studied a model of COVID-19 infection in hamsters and another study by Ogata et al., that detected trace amounts of spike protein in the blood of 12 people who received the Moderna COVID-19 vaccine[5].
As explained in an earlier review, Bridle didn’t account for the vast difference in the level of spike protein present in the hamster model of infection and in vaccinated people. A senior author of the Salk study, Uri Manor, stated on Twitter that the amount in vaccinated people was about 100,000 times lower than in the hamsters:
Congrats to @OgataAlana on this important study. Many asked how much spike protein gets into circulation after vaccination. Turns out to average ~30-40 pg/mL for a few days then disappears.
FYI: This is ~100,000x less than used in our paper (4 ug/mL).https://t.co/k5AChClhI5 pic.twitter.com/xgzJ4RerYG
— Uri Manor 💔 (@manorlaboratory) May 21, 2021
In addition, the biodistribution data, which was obtained in rats and not humans, didn’t show that the lipid nanoparticles were deposited “particularly heavily in the ovaries”. This was also debunked in an earlier review.
In fact, the data showed that the majority of the nanoparticles remained in the injection site, with a peak concentration of 52.8% one hour post-injection. Peak concentrations observed in the brain and ovaries were less than 1%.
And finally, another critical aspect of the biodistribution experiment neglected in the claim is the amount of lipid nanoparticles administered in the rats, which turns out to be irrelevant to the amount present in RNA vaccines given to people, as we explain below.
The study administered 50 micrograms (a microgram is one-millionth of a gram) of lipid nanoparticles to each rat. As explained by David Gorski, a professor of surgery at Wayne State University and editor of Science Based Medicine, this would effectively translate to a much higher dose in rats than in humans. This is due to the large difference in body weight between the two:
“The human vaccine contains […] basically ~0.46 mg lipids or 460 micrograms. Let’s just round it up to 500 μg (0.5 mg). That’s approximately 10x the dose given to the rats. However, for the typical ‘70 kg’ male, 0.5 mg represents a per-weight dose of 0.0071 mg/kg, or 7.1 μg/kg. Let’s compare to the rats, which generally weigh around 200 g (0.2 kg), give or take, at 8 weeks, which is the usual age rodents are used for experiments. That would translate to a per-weight dose of ~250 μg/kg. Even if you used much older rats, who can weigh as much as twice as much, that would still translate to a dose of 125 μg/kg. So we’re looking at a lipid nanoparticle [dose] of ~18-35 times higher (as a rough estimate) than the typical adult human dose.”
In short, the dose used in rats was far higher than that administered to humans.
Claim 8 (Misleading):
“If vaccinated people and unvaccinated people are both carrying the virus, at the same viral loads, then they are both just as likely to infect somebody else. It doesn’t make sense because if you are vaccinated, there is no risk to you from a person who may be unvaccinated.“
It is true that researchers from the U.S. Centers for Disease Control and Prevention reported vaccinated people infected with the Delta variant to carry similar viral loads compared to unvaccinated people, based on PCR testing[6].
But the claim doesn’t account for the fact that vaccinated people are only as likely to infect someone else if they are infected to begin with. Breakthrough infections do occur, but not as often as infections in unvaccinated people. However, an important caveat about our knowledge of breakthrough infections is that it is based primarily on research predating the rise of Delta, although researchers are trying to address the knowledge gap.
At the moment, analyses on vaccine effectiveness against Delta infection have produced conflicting results. A recent report released by the Israeli Ministry of Health found that vaccine effectiveness against infection is just 39%, but it is unclear how many people were included in the analysis.
However, a preprint published on 4 August 2021 by researchers at Imperial College London, examining infections in more than 100,000 people in the community (the REACT study), estimated that vaccines were about 50 to 60% effective at preventing infection.
Still, even if vaccinated people do become infected, they are much less likely to become ill and require hospital care. Indeed, both of the above analyses in Israel and the U.K. found that vaccines remain highly effective at preventing serious illness and hospitalization. A preprint by researchers in Singapore also found that while vaccinated people who are infected can carry similar viral loads as unvaccinated people, the viral load decreases more quickly in the vaccinated. This suggests that they remain infectious for a shorter period of time[7].
On balance, vaccinated people would be less likely to infect others compared to unvaccinated people and less likely to cause an overload of the healthcare system. By and large, the majority of hospitalized COVID-19 patients across the U.S. are unvaccinated, as reported by the New York Times, CNN, and Bloomberg.
The argument that unvaccinated people don’t pose a risk to vaccinated people, and therefore don’t pose a concern, hinges on certain assumptions: 1) everyone who wants to be protected by vaccination already is, 2) the choice not to vaccinate only affects unvaccinated people, and 3) society comprises only two groups, vaccinated people and unvaccinated people who have chosen not to be vaccinated.
But these assumptions are fallacious. They fail to account for the fact that the community has many unvaccinated people who are unvaccinated not because they chose to be, but because they cannot get the vaccine at the moment, and so are forced to rely on those around them for protection (herd immunity). One prominent example is children under 12, as emergency use authorization of the COVID-19 vaccines don’t extend to this age group yet.
And while children in general face a lower risk of serious illness and hospitalization from COVID-19 compared to adults, the sheer rise in the number of infections in this group means that hospitals are seeing an uptick in COVID-19 hospitalizations. Data analyzed by the American Academy of Pediatrics and the Children’s Hospital Association found that children made up nearly 15% of all new COVID-19 cases in the U.S. for the week ending on 5 August 2021. Some hospitals, like those in Texas, ran out of pediatric ICU beds.
Furthermore, some people who are vaccinated don’t receive the full protection from vaccination—those with weakened immune systems, like cancer patients and those who received an organ transplant, are one such example.
Put simply, unvaccinated people who decide not to get vaccinated can affect the health of others around them. Indeed, the nature of infectious diseases is such that public health measures tend to be far more effective if everyone does it, as illustrated in this Twitter thread by Erin Zwiener, a member of the Texas House of Representatives.
🧵 “If you like masks, then nothing’s stop you from wearing one. Just don’t make anyone else.”
What’s wrong with this argument?
Well let’s think about it in terms of an earlier, much simpler and now universally respected public health measure.
Designated latrines.
— Erin Zwiener (@ErinForYall) August 16, 2021
REFERENCES
- 1 – Kory et al. (2021) Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19. American Journal of Therapeutics.
- 2 – Tseng et al. (2021) Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus. PLOS One.
- 3 – Weingartl et al. (2020) Immunization with Modified Vaccinia Virus Ankara-Based Recombinant Vaccine against Severe Acute Respiratory Syndrome Is Associated with Enhanced Hepatitis in Ferrets. Journal of Virology.
- 4 – Lei et al. (2021) SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2. Circulation Research.
- 5 – Ogata et al. (2021) Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clinical Infectious Research.
- 6 – Brown et al. (2021) Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings — Barnstable County, Massachusetts, July 2021. Mortality and Morbidity Weekly Report.
- 7 – Chia et al. (2021) Virological and serological kinetics of SARS-CoV-2 Delta variant vaccine-breakthrough infections: a multi-center cohort study. medRxiv. [Preprint, not peer-reviewed yet.]