- Health
People should take precautions against COVID-19 regardless of their blood type
Key takeaway
Blood type has been linked to risk or protection of various diseases. While a few studies have reported an association between type O blood and a lower incidence of COVID-19 infection, scientists have warned that there is not enough evidence to establish a causal association. Some of the studies used to support the claim that type O blood protects against COVID-19 did not account for certain confounding factors in their analysis, such as pre-existing medical conditions known to influence COVID-19 risk and severity. People should continue to take precautions to prevent infection, regardless of their blood type.
Reviewed content
Verdict:
Claim:
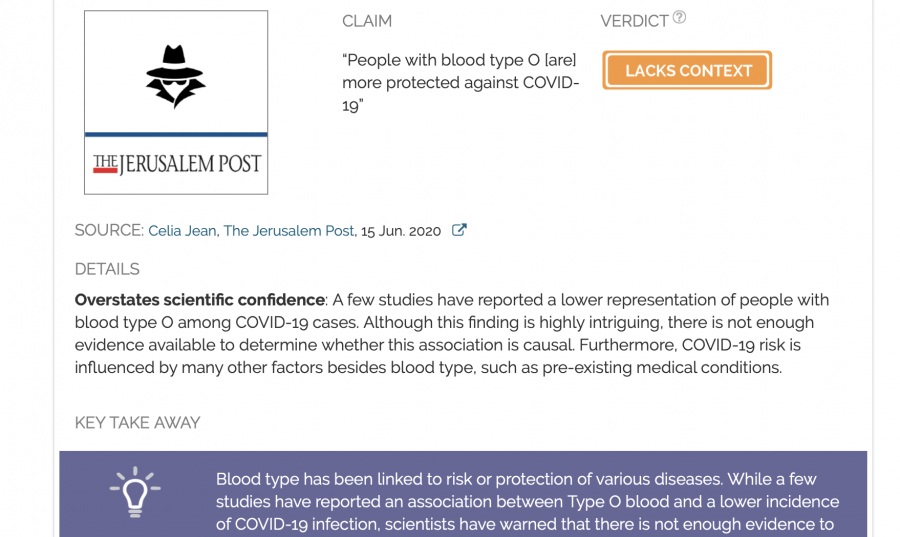
“People with blood type O [are] more protected against COVID-19”
Verdict detail
Overstates scientific confidence: A few studies have reported a lower representation of people with blood type O among COVID-19 cases. Although this finding is highly intriguing, there is not enough evidence available to determine whether this association is causal. Furthermore, COVID-19 risk is influenced by many other factors besides blood type, such as pre-existing medical conditions.
Unsupported: Although the article appears to state this as a fact, the claim that a person with type O blood has antibodies to fight off the virus generated by an infected person with type A blood is a hypothesis that has not yet been validated.
Full Claim
“People with blood type O [are] more protected against COVID-19”; “If a person with blood type A transmits the virus to a person with type O blood, the type O person will have antibodies that can fight the virus.”
Review
An article published in the Jerusalem Post declares that people with type O blood are “more protected against COVID-19”. The article has received more than 23 million views on Facebook and more than 900,000 interactions on the platform since its publication on 15 June. The claim itself had already begun circulating in March 2020 after a preprint (a study that has not yet been peer-reviewed by other scientists) was released by a group of researchers in China. Their study examined blood type prevalence among COVID-19 patients in several Chinese cities, including Wuhan, the original epicenter of the outbreak[1]. The Jerusalem Post article cites this study and others as providing supporting evidence for the claim.
Based on this study, PolitiFact and Snopes fact checked the claim in March 2020; PolitiFact concluded that the study’s findings have not yet been validated and to treat its conclusions with caution, while Snopes found the claim to be unproven. But given that more studies regarding the association between blood type and COVID-19 risk have been published since then, Health Feedback decided to re-examine the newer evidence from four studies cited in the Jerusalem Post article to investigate whether the claim is now substantiated by additional studies. Our analysis finds that the article failed to mention the many caveats and limitations of the recent studies it cites, which exaggerates the certainty and significance of the findings.
1. Zhao et al. MedRxiv[1]
This study formed the basis of the March 2020 claim. It examined blood type prevalence among 1,775 COVID-19 patients (among whom 206 died) at Jinyintan Hospital and 113 patients at Renmin Hospital, both located in Wuhan, Hubei province, as well as 285 patients at Shenzhen Third People’s Hospital, Guangdong province. The prevalence of different blood types among COVID-19 patients was then compared to that of the general population in the respective cities (Wuhan and Shenzhen).
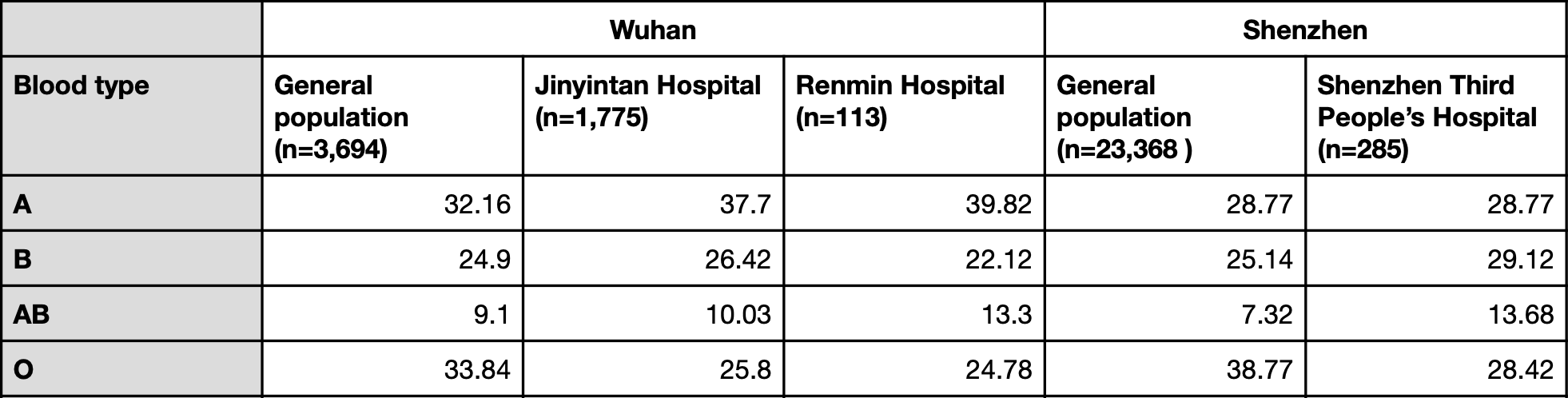
Table 1. Blood type prevalence in the general population and COVID-19 patients in the study (expressed as a percentage).
Based on the differences in blood type prevalence between the general population and hospitalized COVID-19 patients, the authors concluded that the proportion of people with type A blood was significantly higher among COVID-19 patients than in the general population, while the proportion of people with type O blood was significantly lower.
However, looking at the actual figures, we can see that this pattern only holds true in the case of the two Wuhan hospitals, but is not reproduced in the Shenzhen hospital, where blood type AB was overrepresented but blood type A was not. The authors did not explain this discrepancy.
The researchers pointed out that their sample size was small and cautioned that their analysis did not take into account other factors which may influence COVID-19 severity, like pre-existing medical conditions such as chronic obstructive pulmonary disorder, diabetes, and vascular disease.
“It should be emphasized, however, that given the above limitations, it would be premature to use this study to guide clinical practice at this time,” they warned. “Large replication studies with complete information should be encouraged to pursue and are needed to verify the present findings.”
A 17 March article in the South China Morning Post reported comments on the study’s findings by several scientists who were not involved in the research. Yingdai Gao, a researcher with the State Key Laboratory of Experimental Haematology in Tianjin, said that the findings “may be helpful to medical professionals, but ordinary citizens should not take the statistics too seriously.”
People with type A blood should not panic, she said. “It does not mean you will be infected 100 percent,” she said. “If you are type O, it does not mean you are absolutely safe, either. You still need to wash your hands and follow the guidelines issued by authorities.”
Sakthivel Vaiyapuri, an associate professor of cardiovascular & venom pharmacology at the University of Reading, in England, published an article in The Conversation on 24 March 2020, which discussed this preprint’s findings:
“In this observational study, if they considered several other parameters, such as the previous history of other—specifically immune or respiratory-related—diseases, the conclusions might have been different. They have also not explained why they failed to see a significant difference between the blood groups in the Shenzhen hospital. And given [that] COVID-19 is a pandemic, the sample size that they have analysed is not sufficient to draw firm conclusions.”
He warned that more scientific studies were needed to determine the relationship between blood groups and COVID-19. Like Gao, Vaiyapuri also emphasized that people should continue to take precautions to prevent infection, regardless of their blood type.
Tara Moriarty, an associate professor at the University of Toronto who studies infectious diseases, told Snopes that the study provides “an interesting observation that may have an impact on how we identify those most at risk of disease, but until it has been fully peer-reviewed and confirmed/disconfirmed by additional studies, we cannot yet say if blood type affects susceptibility to COVID-19 infection.”
2. Li et al., British Journal of Haematology[2]
This study examined the blood type prevalence of 265 COVID-19 patients at the Central Hospital of Wuhan who had developed pneumonia. Below is the table listing percentages of the prevalence of different blood types at the hospital.
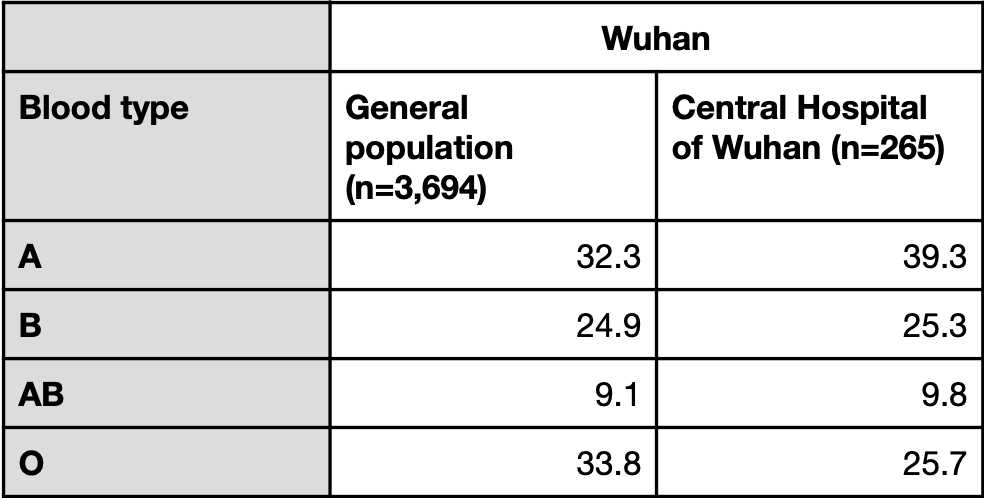
Table 2. Blood type prevalence observed in the general population and in COVID-19 patients with pneumonia at the Central Hospital of Wuhan (expressed in percentages).
In its analysis, the study took into account the data from the two Wuhan hospitals presented in the Zhao et al. study[1], but did not consider data from the Shenzhen hospital. Unlike the Zhao et al. study, Li et al. attempted to eliminate confounding factors, this study did attempt to eliminate confounding factors, such as chronic diseases, although the sample sizes for certain diseases were very small. For example, the authors reported a significantly higher proportion of patients with blood type A who had hepatitis compared to the control group. However, the total number of patients with hepatitis was seven, of which six had blood type A and one had blood type B. Given the very small sample size, the association between blood type A and hepatitis observed in this study may not be meaningful.
The authors concluded that “people with blood group A had a significantly higher risk of SARS‐CoV‐2 infection, whereas blood group O had a significantly lower risk of SARS‐CoV‐2 infection.” However, the sample size for this study is even smaller than in the preprint by Zhao et al., whose findings, as explained earlier, have been called into question by scientists due to its small sample size.
3. Ellinghaus et al., New England Journal of Medicine[3]
This study was conducted in Italy and Spain and involved 1,980 COVID-19 patients from seven hospitals who had been diagnosed with severe COVID-19, which the authors defined as respiratory failure. The researchers conducted a genome-wide association study (GWAS) to identify potential genetic variants associated with the risk of developing severe COVID-19. They found a significant association between severe disease and two different genetic loci (or regions), one of which was located on chromosome 3 and the other on chromosome 9. The region on chromosome 3 spanned six different genes, although the researchers were unable to reliably identify a causative gene with their dataset.
The region on chromosome 9 contains the ABO gene, which codes for an enzyme that converts a protein called the H antigen into A and B antigens. Individuals with blood type O harbor two copies of an ABO gene variant (homozygous) that results in a non-functional enzyme which cannot convert H antigen to A or B antigens. Therefore, people with blood type O cannot produce A or B antigens.
Based on the ABO genotype detected in the GWAS, the researchers inferred the blood type of healthy controls and patients, with the following results:
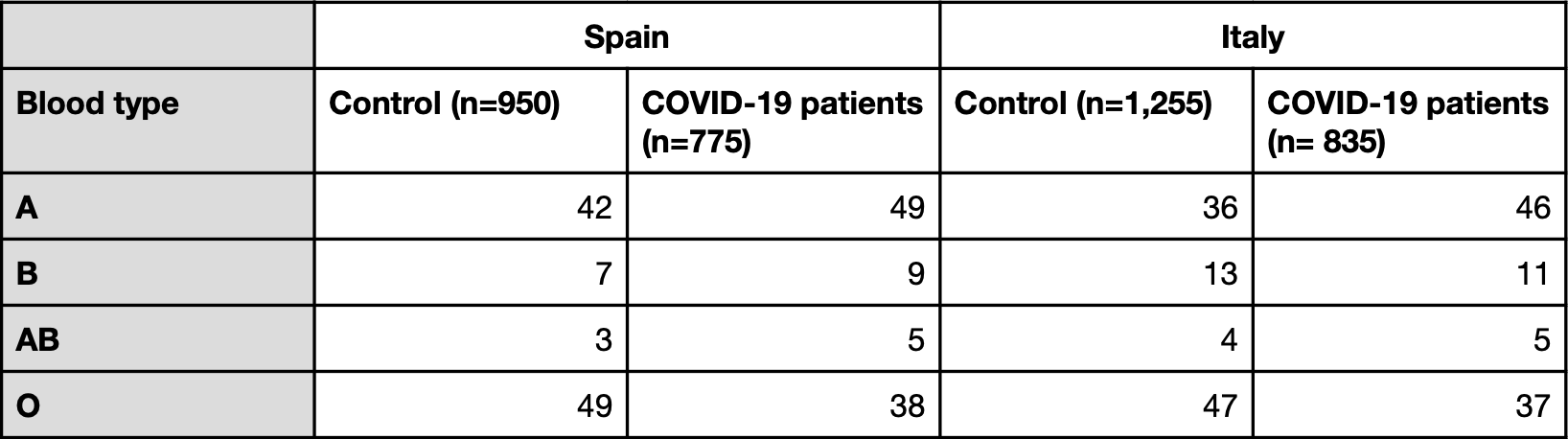
Table 3. Blood type prevalence in the study by Ellinghaus et al. (in percentages)
Similar to what Zhao et al. and Li et al. reported, the blood types showing the greatest differences were A and O, which were more and less represented among COVID-19 patients than in the control population, respectively.
The authors concluded that “Our genetic data confirm that blood group O is associated with a risk of acquiring COVID-19 that was lower than that in non-O blood groups, whereas blood group A was associated with a higher risk than non-A blood groups.”
However, as in the study by Zhao et al., the authors were not able to adjust for confounding factors such as underlying cardiovascular and metabolic issues associated with COVID-19 risk. The authors called for more follow-up studies aimed at identifying potential biological mechanisms and determining the potential of the ABO genotype for profiling COVID-19 risk in patients.
In a CNN report on this study, Roy Silverstein, a professor of medicine at the Medical College of Wisconsin and a hematologist, said that the blood type link was plausible, but that “the absolute difference in risk is very small” and would not be of much importance to the public in general.
“The risk reduction may be statistically significant, but it is a small change in actual risk. You never would tell somebody who was type O that they were at smaller risk of infection,” he said.
4. 23andMe
23andMe is a company that offers consumer genetic testing services. In contrast to the earlier studies discussed in this claim review, the company took a more informal approach in reporting its results. It described in a blog post that among more than 750,000 people who had used 23andMe’s genetic testing service and self-reported as COVID-19 positive, “those with the O blood group were 9-18% less likely to test positive compared to the other groups”.
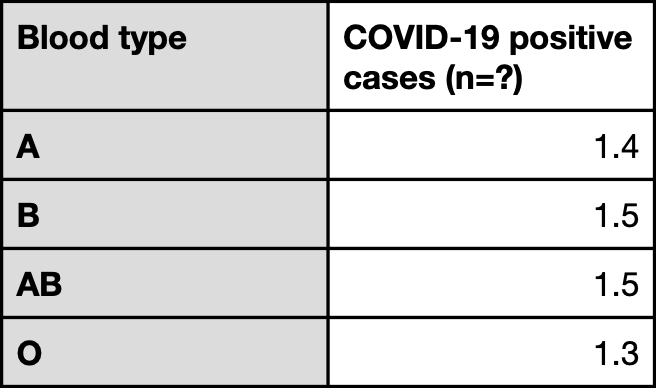
Table 4. Prevalence of different blood types (expressed in percentages) among individuals who used 23andMe’s genetic testing services and self-reported a positive COVID-19 test.
However, unlike the other studies, 23andMe did not sample a representative population that was COVID-19 negative to determine the prevalence of different blood types in the general population. In other words, while the company observed a lower percentage of people with blood type O reporting a positive COVID-19 test relative to people with other blood types, it is not possible to determine whether this is simply due to a lower prevalence of blood type O in the sample population. The results have also not been peer-reviewed by other scientists.
Fumiichiro Yamamoto, an immunohematologist at the Josep Carreras Leukaemia Research Institute in Barcelona, Spain, who is known for his seminal work on the molecular genetic basis of the ABO blood grouping system, told Chemical and Engineering News (C&EN), a publication by the American Chemical Society, that “it’s hard to say much about the 23andMe results because the company did not publish its data.”
Are there known instances of blood type influencing disease risk?
Yes, blood type has been observed to influence the risk of developing certain diseases. For example, this review details how ABO type has been implicated in a higher risk of infection by certain bacteria[4]. The blood type O has also been associated with a greater risk of developing severe cholera[5].
The ABO blood grouping system is the most well-known system, but there are more than 30 other blood grouping systems involving other proteins. This article in The Conversation by Robert Flower, adjunct associate professor at the University of Sydney and a specialist in blood transfusion, discusses the various blood grouping systems, and how the proteins used in one of the systems can provide protection against a form of malaria:
“A blood group known as Duffy is also associated with infection by another type of malaria (known as Plasmodium vivax). When this protein is absent from the red blood cells, the cells are resistant to infection by the malaria parasite. This protein is absent from the blood cells of 90% of sub-Saharan Africans, conferring malaria resistance on this population.”
In terms of COVID-19, although the studies we discussed in this review have reported an association between disease severity and blood type, a biological mechanism that explains a causal association is still lacking.
A group of scientists from INSERM, the French National Institute of Health and Medical Research, have hypothesized that when SARS-CoV-2 infects a cell to produce more virus, it draws on the human host’s own glycan antigens (including A and B antigens, in the case of people with blood types A, B, and AB) when forming its own glycan shield[6]. Because individuals with type O blood form antibodies against A and B antigens, the scientists propose that these antibodies might enable people with type O blood to fight off infection from SARS-CoV-2 generated by individuals with blood types A, B or AB. However, this hypothesis has not been confirmed yet.
Alternatively, Andre Franke, a molecular geneticist at the University of Kiel in Germany and co-author of the Ellinghaus et al. study, speculated in a New York Times article that the chromosome 9 region, which contains the ABO gene, also contains “an on-off switch for a gene producing a protein that triggers strong immune responses,” which might be involved in the immune system’s response to COVID-19.
But the question remains how much protection type O blood might confer against COVID-19. Evidence from the COVID-19 epidemic in the U.S. suggests that any protection or risk that may be associated with blood type is outweighed by the presence or absence of other risk factors.
Laura Cooling, professor and associate director of transfusion medicine at the University of Michigan, highlighted in this C&EN article that “the idea that having type O blood is protective doesn’t match up with the COVID-19’s epidemiology in the U.S. Type O blood is more prevalent among African Americans, yet African Americans have experienced disproportionately high infection rates.”
Indeed, the American Red Cross reports that 51% of African Americans (and 57% of Hispanics) have type O blood, in contrast to 45% of Caucasians, yet African-American and Hispanic communities are disproportionately more affected by COVID-19. A Morbidity and Mortality Weekly report, published by the U.S. Centers for Disease Control and Prevention, found that ethnic minorities are more likely to be affected by COVID-19. Among a sampling of patients hospitalized for COVID-19, 33% were black, compared to 18% in the community[7]. A study by Millett et al. compared COVID-19 cases and deaths between U.S. counties that are disproportionately black—meaning that the percentage of black residents is greater than the national average of 13%—and those counties with less than or equal to 13% black residents. Although only 22% of U.S. counties are disproportionately black, they accounted for 52% of all COVID-19 diagnoses and 58% of all COVID-19 deaths nationally[8].
These observations indicate that blood type alone does not strongly predict COVID-19 protection. As Marcella Nunez-Smith, an associate professor and director of the Equity Research and Innovation Center at the Yale School of Medicine, pointed out in an NPR report: “African-Americans have higher rates of underlying conditions, including diabetes, heart disease, and lung disease, that are linked to more severe cases of COVID-19.” Furthermore, the African-American community is also often affected by reduced access to quality health care and make up a disproportionately higher number of essential frontline workers, meaning that the population overall is more likely to be exposed to the virus.
Therefore, any protection arising from type O blood might be quite small compared to other factors. “It’s what your blood type is, relative to the other person who exposed you, relative to all the other genetic and acquired health conditions you have,” Cooling said.
Conclusion
In summary, a few studies have reported a disproportionately low percentage of people with blood type O among COVID-19 cases relative to their representation in the general population. Although this finding is intriguing and may eventually be useful for identifying patients at risk of severe disease, there is currently not enough evidence available to determine whether a causal association is involved. Some of the studies used to support the claim that type O blood protects against COVID-19 did not take into account certain confounding factors that can influence COVID-19 risk and severity in their analyses, such as pre-existing medical conditions. Therefore, it is not possible to determine whether and how much the findings were influenced by such factors.
The Jerusalem Post article is misleading, as it does not mention the caveats of the research studies it cites nor does it acknowledge that the statement “If a person with blood type A transmits the virus to a person with type O blood, the type O person will have antibodies that can fight the virus” has not been confirmed yet.
Finally, these studies clearly demonstrate that people with blood type O can and do become infected with SARS-CoV-2. Therefore, people should continue to take precautions to avoid infection regardless of their blood type. There are many factors that contribute to COVID-19 infection risk and severity, and scientists have warned that any protective effect that blood type O may confer is likely very small, relative to other factors such as pre-existing medical conditions and socioeconomic background.
REFERENCES
- 1 – Zhao et al. (2020) Relationship between the ABO Blood Group and the COVID-19 Susceptibility. MedRxiv.
- 2 – Li et al. (2020) Association between ABO blood groups and risk of SARS‐CoV‐2 pneumonia. British Journal of Haematology.
- 3 – Ellinghaus et al. (2020) Genomewide Association Study of Severe Covid-19 with Respiratory Failure. New England Journal of Medicine.
- 4 – Cooling L. (2020) Blood Groups in Infection and Host Susceptibility. Clinical Microbiology Reviews.
- 5 – Harris and LaRocque. (2020) Cholera and ABO Blood Group: Understanding an Ancient Association. American Journal of Tropical Medicine and Hygiene.
- 6 – Breiman et al. (2020) Harnessing the natural anti-glycan immune response to limit the transmission of enveloped viruses such as SARS-CoV-2. PLoS Pathogens.
- 7 – Garg et al. (2020) Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019 — COVID-NET, 14 States, March 1–30, 2020. MMWR Morbidity and Mortality Weekly Report.
- 8 – Millett et al. (2020) Assessing Differential Impacts of COVID-19 on Black Communities. Annals of Epidemiology.